
Acute vs chronic management — MCQs

A 32-year-old woman comes to the office for a regular follow-up. She was diagnosed with type 2 diabetes mellitus 4 years ago. Her last blood test showed a fasting blood glucose level of 6.6 mmol/L (118.9 mg/dL) and HbA1c of 5.1%. No other significant past medical history. Current medications are metformin and a daily multivitamin. No significant family history. The physician wants to take her blood pressure measurements, but the patient states that she measures it every day in the morning and in the evening and even shows him a blood pressure diary with all the measurements being within normal limits. Which of the following statements is correct?
A 28-year-old soldier is brought back to a military treatment facility 45 minutes after sustaining injuries in a building fire from a mortar attack. He was trapped inside the building for around 20 minutes. On arrival, he is confused and appears uncomfortable. He has a Glasgow Coma Score of 13. His pulse is 113/min, respirations are 18/min, and blood pressure is 108/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. Examination shows multiple second-degree burns over the chest and bilateral upper extremities and third-degree burns over the face. There are black sediments seen within the nose and mouth. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. Intravenous fluid resuscitation is begun. Which of the following is the most appropriate next step in management?
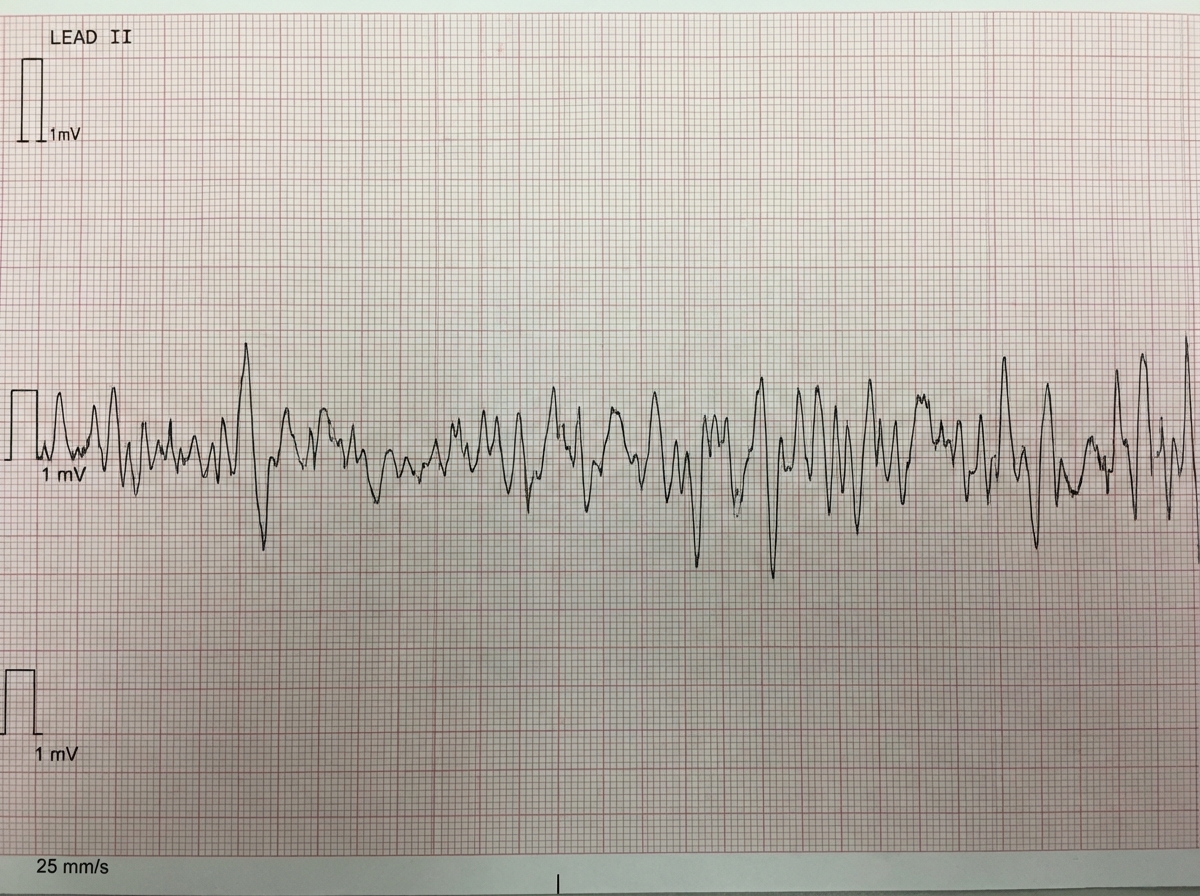
One hour after being admitted to the hospital for sharp, acute chest pain and diaphoresis, a 55-year-old woman with type 2 diabetes mellitus loses consciousness in the emergency department. There are no palpable pulses. Chest compressions are started. The patient has a history of breast cancer that was surgically treated 4 years ago. Prior to admission, the patient was on a long bus ride to visit her sister. Her medications include tamoxifen, atorvastatin, metoprolol, metformin, and insulin. Serum troponin levels are elevated. The cardiac rhythm is shown. Which of the following is the most appropriate next step in management?
A 55-year-old man presents to his primary care physician for a wellness checkup. He states that he generally feels well and has no complaints at this time. The patient consumes alcohol frequently, eats a high sodium diet, and is sedentary. His temperature is 97.5°F (36.4°C), blood pressure is 167/108 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 99% on room air. The patient is 5'10" tall and weighs 220 lbs (BMI 31.5 kg/m²). The patient's blood pressure at his last 2 appointments were 159/100 mmHg and 162/99 mmHg, respectively. His physician wants to intervene to manage his blood pressure. Which of the following is the most effective lifestyle intervention for this patient's hypertension?
A 64-year-old woman is brought to the emergency department 1 hour after the onset of acute shortness of breath and chest pain. The chest pain is retrosternal in nature and does not radiate. She feels nauseated but has not vomited. She has type 2 diabetes mellitus, hypertension, and chronic kidney disease. Current medications include insulin, aspirin, metoprolol, and hydrochlorothiazide. She is pale and diaphoretic. Her temperature is 37°C (98°F), pulse is 136/min, and blood pressure is 80/60 mm Hg. Examination shows jugular venous distention and absence of a radial pulse during inspiration. Crackles are heard at the lung bases bilaterally. Cardiac examination shows distant heart sounds. Laboratory studies show: Hemoglobin 8.3 g/dL Serum Glucose 313 mg/dL Urea nitrogen 130 mg/dL Creatinine 6.0 mg/dL Which of the following is the most appropriate next step in management?
A 57-year-old woman with type 2 diabetes mellitus comes to the physician for a follow-up examination. She previously had been compliant with her diet and medication but has had a 5-kg (11-lb) weight gain since the last visit 6 months ago. She reports that she often misses doses of her metformin. Her hemoglobin A1c is 9.8%. Which of the following is the most appropriate course of action?
A 72-year-old man presents to the emergency department after a fall. The patient was found lying down on the floor in his room in his retirement community. The patient has a past medical history of Alzheimer dementia and a prosthetic valve. His current medications include donepezil and warfarin. His temperature is 97.7°F (36.5°C), blood pressure is 85/50 mmHg, pulse is 160/min, respirations are 13/min, and oxygen saturation is 97% on room air. The patient is started on IV fluids and a type and screen is performed. Laboratory values are ordered as seen below. Hemoglobin: 13 g/dL Hematocrit: 39% Leukocyte count: 5,500 cells/mm^3 with normal differential Platelet count: 225,000/mm^3 INR: 2.5 AST: 10 U/L ALT: 12 U/L A chest radiograph and EKG are performed and are within normal limits. A full physical exam is within normal limits. The patient's vitals are repeated. His temperature is 99.5°F (37.5°C), blood pressure is 110/70 mmHg, pulse is 90/min, respirations are 10/min, and oxygen saturation is 98% on room air. Which of the following is the best next step in management?
A 55-year-old man presents to the emergency department with hematemesis that started 1 hour ago but has subsided. His past medical history is significant for cirrhosis with known esophageal varices which have been previously banded. His temperature is 97.5°F (36.4°C), blood pressure is 114/64 mmHg, pulse is 130/min, respirations are 12/min, and oxygen saturation is 98% on room air. During the patient's physical exam, he begins vomiting again and his heart rate increases with a worsening blood pressure. He develops mental status changes and on exam he opens his eyes and flexes his arms only to sternal rub and is muttering incoherent words. Which of the following is the most appropriate next step in management?
A 52-year-old woman presents to the clinic with several days of vomiting and diarrhea. She also complains of headaches, muscle aches, and fever, but denies tenesmus, urgency, and bloody diarrhea. Past medical history is insignificant. When asked about any recent travel she says that she just came back from a cruise ship vacation. Her temperature is 37°C (98.6° F), respiratory rate is 15/min, pulse is 67/min, and blood pressure is 122/98 mm Hg. Physical examination is non-contributory. Microscopic examination of the stool is negative for ova or parasites. What is the most likely diagnosis?
A 55-year-old man comes to the physician because of a 4-month history of episodic, pressure-like chest pain. The chest pain occurs when he is walking up stairs and improves with rest. He has hypertension and type 2 diabetes mellitus. His father died from a myocardial infarction at the age of 50 years. Current medications include hydrochlorothiazide and metformin. His pulse is 85/min, respirations are 12/min, and blood pressure is 140/90 mm Hg. Cardiac examination shows normal heart sounds without any murmurs, rubs, or gallops. An ECG shows high amplitude of the S wave in lead V3. An exercise stress test is performed but stopped after 4 minutes because the patient experiences chest pain. An ECG obtained during the stress test shows sinus tachycardia and ST-segment depressions in leads V1–V4. Which of the following is the most appropriate long-term pharmacotherapy to reduce the frequency of symptoms in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app