
Sensitivity/Specificity — MCQs

On this page
A new real time-PCR test for the hepatitis C virus is approved for medical use. The manufacturer sets the threshold number of DNA copies required to achieve a positive result such that the sensitivity is 98% and the specificity is 80%. The tested population has a hepatitis C prevalence of 0.7%. Which of the following changes in the prevalence, incidence, or threshold concentration will increase the positive predictive value of the test, if the other two values are held constant?
A 36-year-old female presents to clinic inquiring about the meaning of a previous negative test result from a new HIV screening test. The efficacy of this new screening test for HIV has been assessed by comparison against existing gold standard detection of HIV RNA via PCR. The study includes 1000 patients, with 850 HIV-negative patients (by PCR) receiving a negative test result, 30 HIV-negative patients receiving a positive test result, 100 HIV positive patients receiving a positive test result, and 20 HIV positive patients receiving a negative test result. Which of the following is most likely to increase the negative predictive value for this test?
A novel PET radiotracer is being evaluated for its ability to aid in the diagnosis of Alzheimer’s disease (AD). The study decides to use a sample size of 1,000 patients, and half of the patients enrolled have AD. In the group of patients with AD, 400 are found positive on the novel type of PET imaging examination. In the control group, 50 are found positive. What is the PPV of this novel exam?
A new assay for Lyme disease has been developed. While the assay has been tested extensively in Maine, a group of inventors are planning to test it in Southern California. In comparison to the assay's performance in Maine, testing the assay in Southern California would affect the performance of the assay in which of the following ways?
A genetic population study is being conducted to find the penetrance of a certain disease. This disease is associated with impaired iron metabolism and primarily affects the liver. Patients often present with diabetes and bronze skin pigmentation. After a genetic screening of 120 inhabitants with a family history of this disease, 40 were found to have the disease-producing genotype, but only 10 presented with symptoms. What are the chances of the screened patients with said genotype developing the disease phenotype?
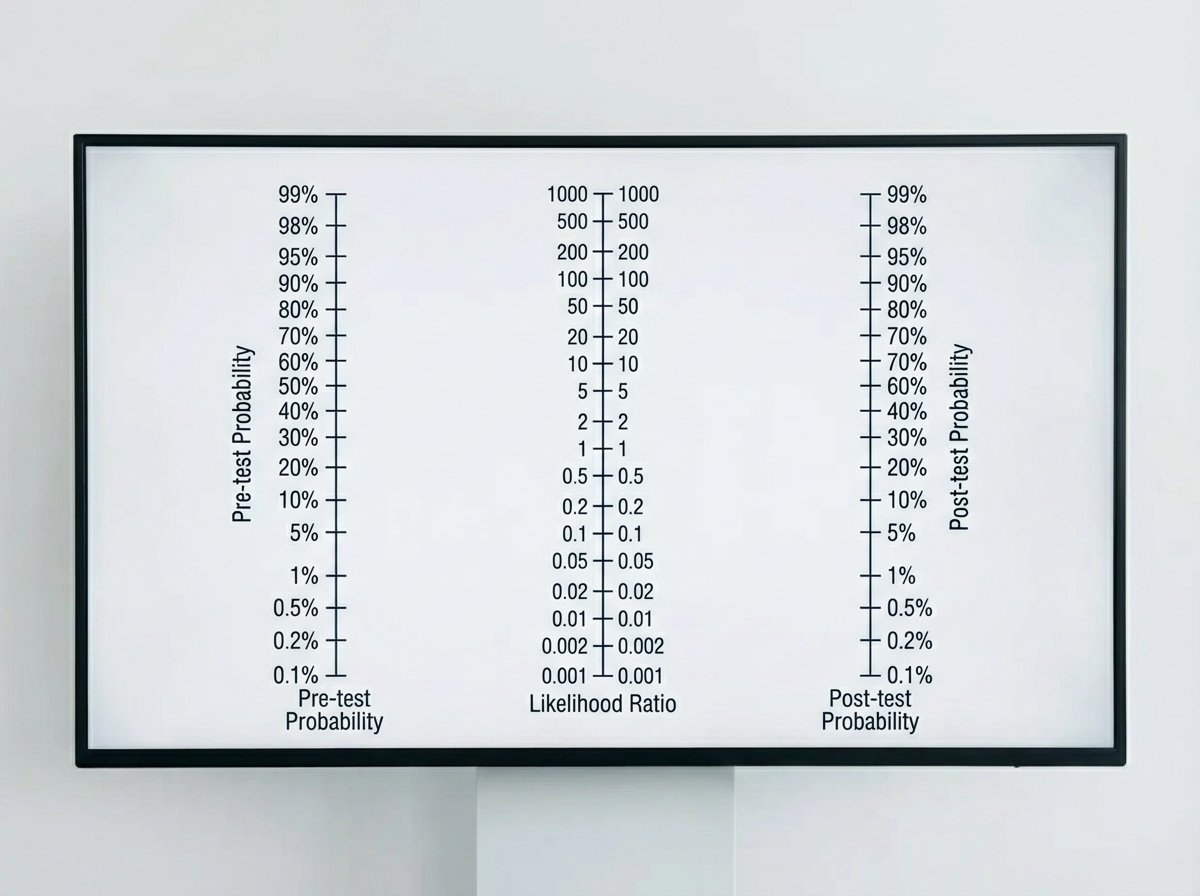
A 14-month-old boy is brought in by his parents with an 8-month history of diarrhea, abdominal tenderness and concomitant failure to thrive. The pediatric attending physician believes that Crohn’s disease is the best explanation of this patient’s symptoms. Based on the pediatric attending physician’s experience, the pretest probability of this diagnosis is estimated at 40%. According to Fagan nomogram (see image). If the likelihood ratio of a negative test result (LR-) for Crohn’s disease is 0.04, what is the chance that this is the correct diagnosis in this patient with a negative test result?
A geriatric investigator is evaluating the consistency of Alzheimer dementia diagnoses based on clinical symptoms. Patients with known chart diagnoses of Alzheimer dementia were evaluated by multiple physicians during a fixed time interval. Each evaluator was blinded to the others' assessments. The extent to which the diagnosis by one physician was replicated by another clinician examining the same patient is best described by which of the following terms?
An infectious disease investigator is evaluating the diagnostic accuracy of a new interferon-gamma-based assay for diagnosing tuberculosis in patients who have previously received a Bacillus Calmette-Guérin (BCG) vaccine. Consenting participants with a history of BCG vaccination received an interferon-gamma assay and were subsequently evaluated for tuberculosis by sputum culture. Results of the study are summarized in the table below. Tuberculosis, confirmed by culture No tuberculosis Total Positive interferon-gamma assay 90 6 96 Negative interferon-gamma assay 10 194 204 Total 100 200 300 Based on these results, what is the sensitivity of the interferon-gamma-based assay for the diagnosis of tuberculosis in this study?
You are reviewing raw data from a research study performed at your medical center examining the effectiveness of a novel AIDS screening examination. The study enrolled 250 patients with confirmed AIDS, and 240 of these patients demonstrated a positive screening examination. The control arm of the study enrolled 250 patients who do not have AIDS, and only 5 of these patients tested positive on the novel screening examination. What is the NPV of this novel test?
A new screening test utilizing a telemedicine approach to diagnosing diabetic retinopathy has been implemented in a diabetes clinic. An ophthalmologist’s exam was also performed on all patients as the gold standard for diagnosis. In a pilot study of 500 patients, the screening test detected the presence of diabetic retinopathy in 250 patients. Ophthalmologist exam confirmed a diagnosis of diabetic retinopathy in 200 patients who tested positive in the screening test, as well as 10 patients who tested negative in the screening test. What is the sensitivity, specificity, positive predictive value, and negative predictive value of the screening test?
Practice by Chapter
Definitions and calculations
Practice Questions
2x2 contingency tables
Practice Questions
Relationship with false positive/negative rates
Practice Questions
Positive predictive value (PPV)
Practice Questions
Negative predictive value (NPV)
Practice Questions
Effect of disease prevalence on predictive values
Practice Questions
Likelihood ratios
Practice Questions
ROC curve analysis
Practice Questions
Area under the curve (AUC) interpretation
Practice Questions
Optimizing cut-off values
Practice Questions
Trade-offs between sensitivity and specificity
Practice Questions
Multi-test algorithms
Practice Questions
Application to screening programs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app