
Sensitivity/Specificity — MCQs

On this page
A public health campaign increases vaccination rates against human papillomaviruses 16 and 18. Increased vaccination rates would have which of the following effects on the Papanicolaou test?
A pharmaceutical corporation is developing a research study to evaluate a novel blood test to screen for breast cancer. They enrolled 800 patients in the study, half of which have breast cancer. The remaining enrolled patients are age-matched controls who do not have the disease. Of those in the diseased arm, 330 are found positive for the test. Of the patients in the control arm, only 30 are found positive. What is this test’s sensitivity?
A scientist in Boston is studying a new blood test to detect Ab to the parainfluenza virus with increased sensitivity and specificity. So far, her best attempt at creating such an exam reached 82% sensitivity and 88% specificity. She is hoping to increase these numbers by at least 2 percent for each value. After several years of work, she believes that she has actually managed to reach a sensitivity and specificity even greater than what she had originally hoped for. She travels to South America to begin testing her newest blood test. She finds 2,000 patients who are willing to participate in her study. Of the 2,000 patients, 1,200 of them are known to be infected with the parainfluenza virus. The scientist tests these 1,200 patients’ blood and finds that only 120 of them tested negative with her new test. Of the following options, which describes the sensitivity of the test?
A 26-year-old medical student comes to the physician with a 3-week history of night sweats and myalgias. During this time, he has also had a 3.6-kg (8-lb) weight loss. He returned from a 6-month tropical medicine rotation in Cambodia 1 month ago. A chest x-ray (CXR) shows reticulonodular opacities suggestive of active tuberculosis (TB). The student is curious about his likelihood of having active TB. He reads a study that compares sputum testing results between 2,800 patients with likely active TB on a basis of history, clinical symptoms, and CXR pattern and 2,400 controls. The results are shown: Sputum testing positive for TB Sputum testing negative for TB Total Active TB likely on basis of history, clinical symptoms, and CXR pattern 700 2100 2,800 Active TB not likely on basis of history, clinical symptoms, and CXR pattern 300 2100 2,400 Total 1000 4200 5,200 Which of the following values reflects the probability that a patient with a diagnosis of active TB on the basis of history, clinical symptoms, and CXR pattern actually has active TB?
A 1-year-old boy is brought to the emergency room by his parents because of inconsolable crying and diarrhea for the past 6 hours. As the physician is concerned about acute appendicitis, she consults the literature base. She finds a paper with a table that summarizes data regarding the diagnostic accuracy of multiple clinical findings for appendicitis: Clinical finding Sensitivity Specificity Abdominal guarding (in children of all ages) 0.70 0.85 Anorexia (in children of all ages) 0.75 0.50 Abdominal rebound (in children ≥ 5 years of age) 0.85 0.65 Vomiting (in children of all ages) 0.40 0.63 Fever (in children from 1 month to 2 years of age) 0.80 0.80 Based on the table, the absence of which clinical finding would most accurately rule out appendicitis in this patient?
Health officials are considering making a change to the interpretation of the tuberculin skin test that will change the cut-off for a positive purified protein derivative (PPD) from 10 mm to 15 mm for healthcare workers. Which of the following can be expected as a result of this change?
A 17-year-old girl comes to the urgent care center after testing negative for HIV. She recently had sexual intercourse for the first time and had used a condom with her long-term boyfriend. She has no personal history of serious illness and no history of sexually transmitted infections. However, the patient is still worried about the possibility she has HIV despite the negative HIV test. She states that the package insert of the HIV test shows that of 100 patients who are found to be HIV-positive on PCR, 91 tested positive via the HIV test. Later in the day, a 23-year-old woman with a history of genitourinary chlamydia infection also comes to the urgent care center after testing negative for HIV. She states that she recently had unprotected intercourse with “someone who might have HIV.” If the test is conducted a second time on the 23-year-old patient, how will its performance compare to a second test conducted on the 17-year-old patient?
An at-home recreational drug screening test kit is currently being developed. They consult you for assistance with determining an ideal cut-off point for the level of the serum marker in the test kit. This cut-off point will determine what level of serum marker is associated with a positive or negative test, with serum marker levels greater than the cut-off point indicative of a positive test and vice-versa. The cut-off level is initially set at 4 mg/uL, which is associated with a sensitivity of 92% and a specificity of 97%. How will the sensitivity and specificity of the test change if the cut-off level is raised to 6 mg/uL?
A medical research study is beginning to evaluate the positive predictive value of a novel blood test for non-Hodgkin’s lymphoma. The diagnostic arm contains 700 patients with NHL, of which 400 tested positive for the novel blood test. In the control arm, 700 age-matched control patients are enrolled and 0 are found positive for the novel test. What is the PPV of this test?
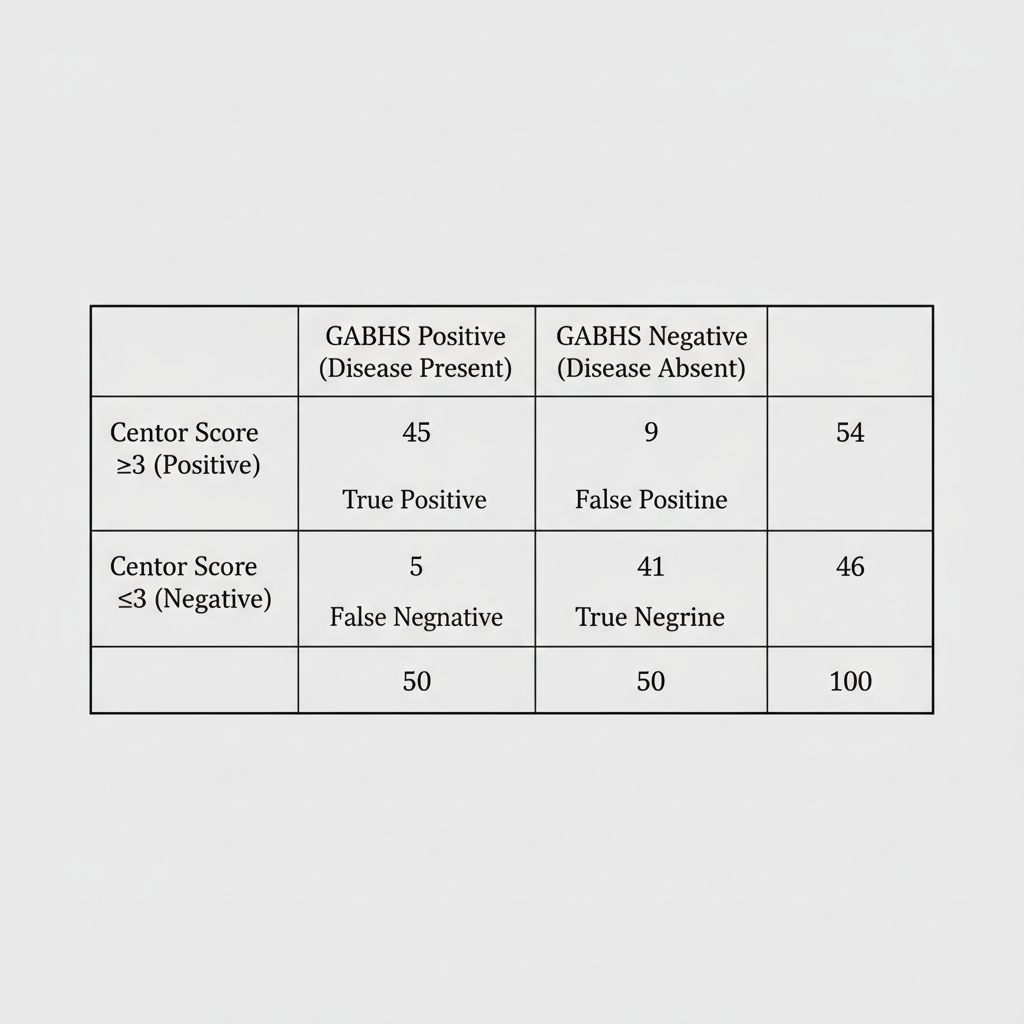
A 16-year-old female is seen at her outpatient primary medical doctor's office complaining of a sore throat. Further history reveals that she has no cough and physical exam is notable for tonsillar exudates. Vitals in the office reveal HR 88, RR 16, and T 102.1. Using the Centor criteria for determining likelihood of Group A beta-hemolytic strep pharyngitis, the patient has a score of 3. A review of the primary literature yields the findings in Image A. What is the specificity of the Centor criteria using a score of 3 as a cutoff value?
Practice by Chapter
Definitions and calculations
Practice Questions
2x2 contingency tables
Practice Questions
Relationship with false positive/negative rates
Practice Questions
Positive predictive value (PPV)
Practice Questions
Negative predictive value (NPV)
Practice Questions
Effect of disease prevalence on predictive values
Practice Questions
Likelihood ratios
Practice Questions
ROC curve analysis
Practice Questions
Area under the curve (AUC) interpretation
Practice Questions
Optimizing cut-off values
Practice Questions
Trade-offs between sensitivity and specificity
Practice Questions
Multi-test algorithms
Practice Questions
Application to screening programs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app