
Molecular Genetics — MCQs

On this page
An 11-month-old boy is brought to the physician by his adoptive mother for the evaluation of seizures and musty-smelling urine. His immunizations are up-to-date. His height and weight are both below the 10th percentile. He is pale and has blue eyes. He cannot pull himself up from a seated position to stand and does not crawl. Which of the following genetic principles best explains the variety of phenotypic traits seen in this patient?
A 4-year-old boy is brought to the pediatrician by his mother for a routine medical examination. His medical history is relevant for delayed gross motor milestones. The mother is concerned about a growth delay because both of his brothers were twice his size at this age. Physical examination reveals a well-groomed and healthy boy with a prominent forehead and short stature, in addition to shortened upper and lower extremities with a normal vertebral column. The patient’s vitals reveal: temperature 36.5°C (97.6°F); pulse 60/min; and respiratory rate 17/min and a normal intelligence quotient (IQ). A mutation in which of the following genes is the most likely cause underlying the patient’s condition?
A 12-hour old male infant is seen in the newborn nursery. He was born full term by vaginal delivery to a 40-year-old G4P3-->4 mother. Her pregnancy and delivery were uncomplicated, notable only for declining genetic testing. On exam, her son has a flat face, a fold in the upper eyelid, palpebral fissures that appear to slant upwards, and small ears. The diagnostic test for her son’s most likely condition should be conducted during which of the following phases of the cell cycle?
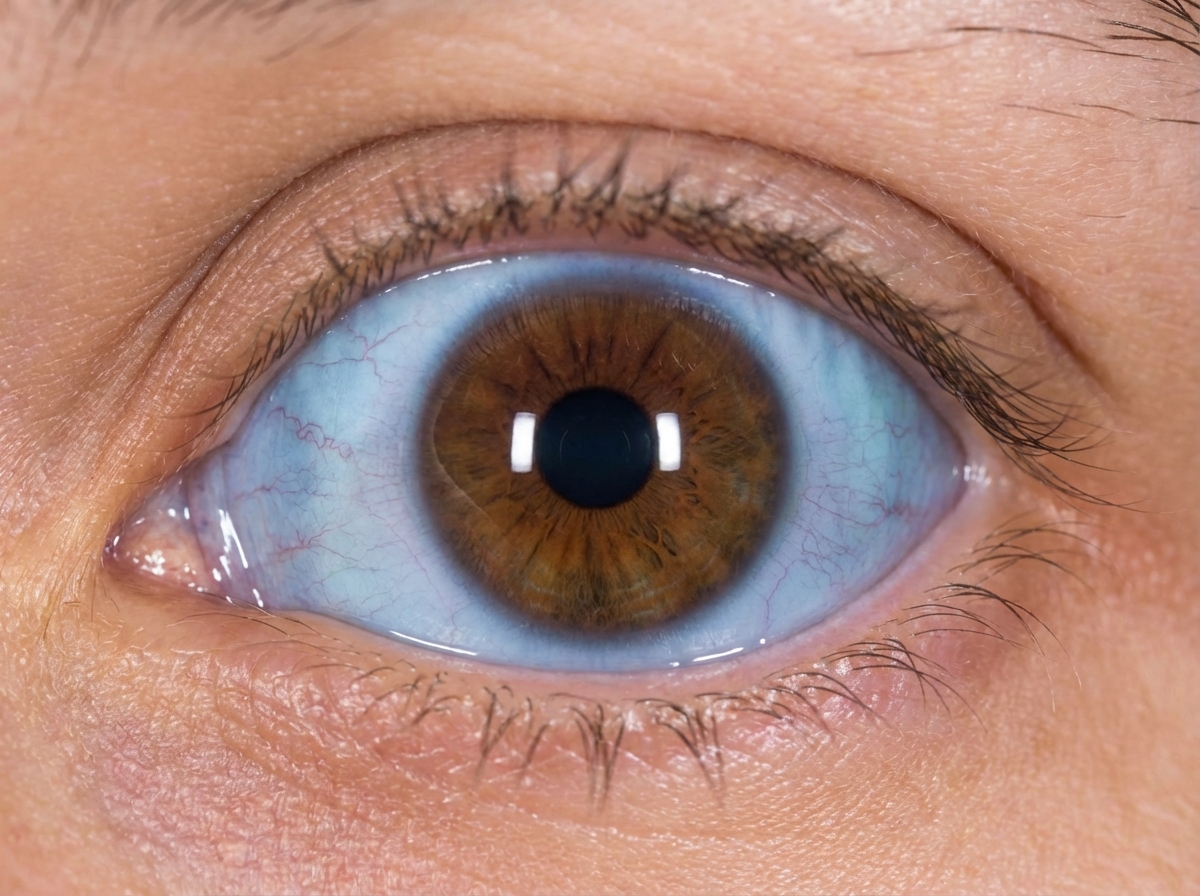
A 7-year-old girl presents to her primary care physician for a routine check-up. The physician allows the medical student to perform a physical examination. The medical student notes hearing impairment as well as the findings show in Figure A. Radiographs show indications of multiple old fractures of the humerus that have healed. After questioning the girl's parents, the medical student learns that in addition, the patient is extremely picky with her food and eats a diet consisting mainly of cereal and pasta. What is the most likely etiology of the patient's disease?
An investigator is studying human genetics and cell division. A molecule is used to inhibit the exchange of genetic material between homologous chromosomes. Which of the following phases of the cell cycle does the molecule target?
A 2-month-old boy is brought to the physician by his mother because of poor weight gain and irritability since delivery. He is at the 10th percentile for height and below the 5th percentile for weight. Physical examination shows conjunctival pallor. Laboratory studies show: Hemoglobin 11.2 g/dL Mean corpuscular hemoglobin 24.2 pg/cell Mean corpuscular volume 108 μm3 Serum Ammonia 26 μmol/L (N=11–35 μmol/L) A peripheral blood smear shows macrocytosis of erythrocytes and hypersegmented neutrophils. Supplementation with folate and cobalamin is begun. Two months later, his hemoglobin concentration is 11.1 g/dL and mean corpuscular volume is 107 μm3. The patient's condition is most likely caused by failure of which of the following enzymatic reactions?
Red-green color blindness, an X-linked recessive disorder, has an incidence of 1/200 in males in a certain population. What is the probability of a phenotypically normal male and female having a child with red-green color blindness?
A 9-month-old female is brought to the emergency department after experiencing a seizure. She was born at home and was normal at birth according to her parents. Since then, they have noticed that she does not appear to be achieving developmental milestones as quickly as her siblings, and often appears lethargic. Physical exam reveals microcephaly, very light pigmentation (as compared to her family), and a "musty" body odor. The varied manifestations of this disease can most likely be attributed to which of the following genetic principles?
Practice by Chapter
DNA structure and organization
Practice Questions
Chromosomal structure
Practice Questions
DNA replication
Practice Questions
Cell cycle and mitosis
Practice Questions
Meiosis and genetic recombination
Practice Questions
Mutation types and consequences
Practice Questions
Mendelian inheritance patterns
Practice Questions
Non-Mendelian inheritance
Practice Questions
Genetic linkage and mapping
Practice Questions
Population genetics principles
Practice Questions
Genetic polymorphisms
Practice Questions
Gene therapy approaches
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app