
Metabolism — MCQs

On this page
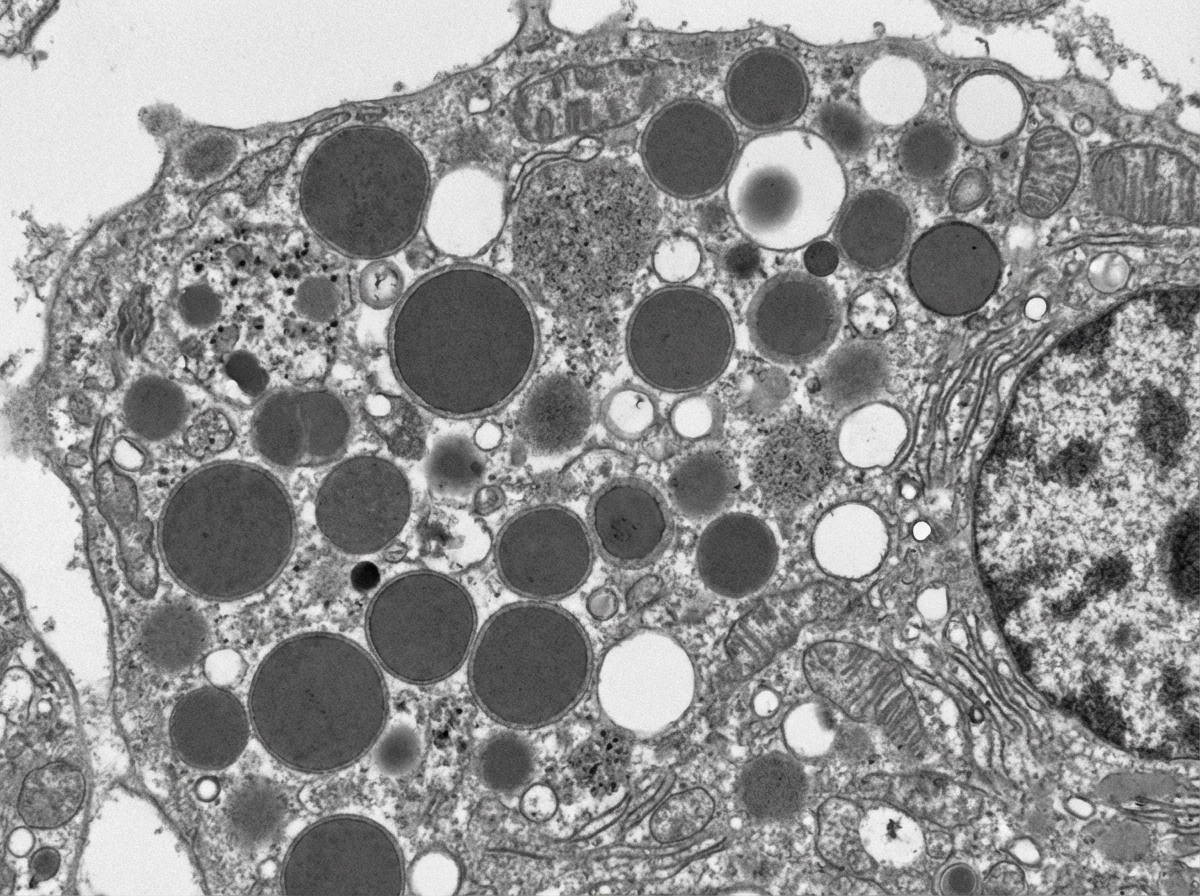
A 3-month-old boy presents for routine health maintenance. The patient has coarse facial features and stiff joint movements with restricted passive and active range of motion. He also has problems following objects with his eyes and seems not to focus on anything. On physical examination, the corneas are clouded, and the patient fails to meet any 3-month developmental milestones. Genetic testing and histopathology are performed and reveal failure of a cellular structure to phosphorylate mannose residues on glycoproteins. An electron microscopy image of one of this patient’s cells is shown. Which of the following is the most likely diagnosis in this patient?
A 6-day-old infant who was born via uncomplicated vaginal delivery at 39 weeks of gestation is brought to the family physician for poor feeding. The mother received adequate prenatal care throughout the pregnancy, and has no medical conditions. On physical exam, the infant's temperature is 36.5°C (97.7°F), blood pressure is 70/45 mmHg, pulse is 170/min, and respirations are 40/min. The infant has dry mucous membranes, capillary refill of 4 seconds, and a depressed anterior fontanelle. No abdominal masses are noted. Genital exam shows enlargement of the clitoris with fusion of the labioscrotal folds. Serum chemistry is remarkable for hyponatremia and hyperkalemia. The infant's karyotype is 46,XX. Which of the following findings are most likely to be discovered upon further workup?
A 7-month-old boy is brought to the pediatrician for a change in his behavior. The patient has been exclusively breastfeeding up until this point and has been meeting his developmental milestones. He is in the 90th percentile for weight and 89th percentile for height. Two weeks ago, his parents began introducing weaning foods including fruit purees and baby formula. This past week, the patient has been increasingly lethargic, vomiting, and has been refusing to eat. The patient's parents state that he had an episode this morning where he was not responsive and was moving his extremities abnormally followed by a period of somnolence. The patient's past medical history is notable for shoulder dystocia and poorly managed maternal diabetes during the pregnancy. His temperature is 99.5°F (37.5°C), blood pressure is 60/30 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. On physical exam, you note a lethargic infant with a distinctive sweet, fruity smell to his breath. Which of the following is most likely deficient in this patient?
A 35-year-old man presents to the general practitioner with a skin rash that has been present for 2 days. The rash appeared suddenly and has progressively gotten worse. It started off as an erythematous lesion on the back of his hands and also over his nose. The lesions over his hands have become bullous and tense. He has never experienced similar symptoms before. He just got back from a canoeing trip during a very hot and sunny weekend. Physical exam is significant for erythematous, vesicular lesions over the nape of the neck and bridge of the nose as well as tense bullae over the dorsum of both hands. The attending physician suspects a defect in the synthesis of heme and orders some blood tests. Which of the following precursors will most likely be elevated in this patient?
A 17-year-old girl with a BMI of 14.5 kg/m2 is admitted to the hospital for the treatment of anorexia nervosa. The patient is administered intravenous fluids and is supplied with 1,600 calories daily with an increase of 200 calories each day. On day 5 of treatment, the patient manifests symptoms of weakness and confusion, and dark brown urine. Which of the following clinical conditions is the most likely cause of the patient's symptoms?
A 28-year-old woman comes to the emergency department because of a 2-day history of dark urine, increasing abdominal pain, and a tingling sensation in her arms and legs. She has a history of epilepsy. Her current medication is phenytoin. She is nauseated and confused. Following the administration of hemin and glucose, her symptoms improve. The beneficial effect of this treatment is most likely due to inhibition of which of the following enzymes?
A 35-year-old woman comes to the physician because of a 1-day history of swelling and pain in the left leg. Two days ago, she returned from a business trip on a long-distance flight. She has alcohol use disorder. Physical examination shows a tender, swollen, and warm left calf. Serum studies show an increased homocysteine concentration and a methylmalonic acid concentration within the reference range. Further evaluation of this patient is most likely to show which of the following serum findings?
A 41-year-old African American woman presents with her husband to her primary care doctor for evaluation of depression and anxiety. She reports a 2-week history of rapid onset sadness with no clear inciting factor. She is accompanied by her husband who notes that she has had at least three similar episodes that have occurred over the past two years. He also notes that she has been “more emotional” lately and seems confused throughout the day. She has had to leave her job as a librarian at her child’s elementary school. Her past medical history is notable for two diagnostic laparoscopies for recurrent episodes of abdominal pain of unknown etiology. Her family history is notable for psychosis in her mother and maternal grandfather. Her temperature is 99°F (37.2°C), blood pressure is 125/75 mmHg, pulse is 75/min, and respirations are 17/min. On exam, she is disheveled and appears confused and disoriented. Her attention span is limited and she exhibits emotional lability. This patient’s condition is most likely due to a defect in an enzyme that metabolizes which of the following compounds?
A 5-year-old male visits his pediatrician for a check-up. His height corresponds to the 99th percentile for his age, and pubic hair is present upon physical examination. Serum renin and potassium levels are high, as is 17-hydroxyprogesterone. Which of the following is likely deficient in this patient?
A 38-year-old man presents to his physician with double vision persisting for a week. When he enters the exam room, the physician notes that the patient has a broad-based gait. The man’s wife informs the doctor that he has been an alcoholic for the last 5 years and his consumption of alcohol has increased significantly over the past few months. She also reports that he has become indifferent to his family members over time and is frequently agitated. She also says that his memory has been affected significantly, and when asked about a particular detail, he often recollects it incorrectly, though he insists that his version is the true one. On physical examination, his vital signs are stable, but when the doctor asks him where he is, he seems to be confused. His neurological examination also shows nystagmus. Which of the following options describes the earliest change in the pathophysiology of the central nervous system in this man?
Practice by Chapter
TCA cycle reactions and regulation
Practice Questions
Electron transport chain and oxidative phosphorylation
Practice Questions
Pentose phosphate pathway
Practice Questions
Gluconeogenesis
Practice Questions
Glycogen metabolism
Practice Questions
Amino acid metabolism
Practice Questions
Integration of metabolic pathways
Practice Questions
Fed state vs. fasting state metabolism
Practice Questions
Exercise metabolism
Practice Questions
Alcohol metabolism
Practice Questions
Metabolic adaptations in starvation
Practice Questions
Metabolic disorders overview
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app