
Metabolism — MCQs

On this page
An otherwise healthy 45-year-old woman comes to the physician because of a 1-year history of episodic abdominal cramps, bloating, and flatulence. The symptoms worsen when she consumes pizza or ice cream and have become more frequent over the past 4 months. Lactose intolerance is suspected. Which of the following would most strongly support the diagnosis of lactose intolerance?
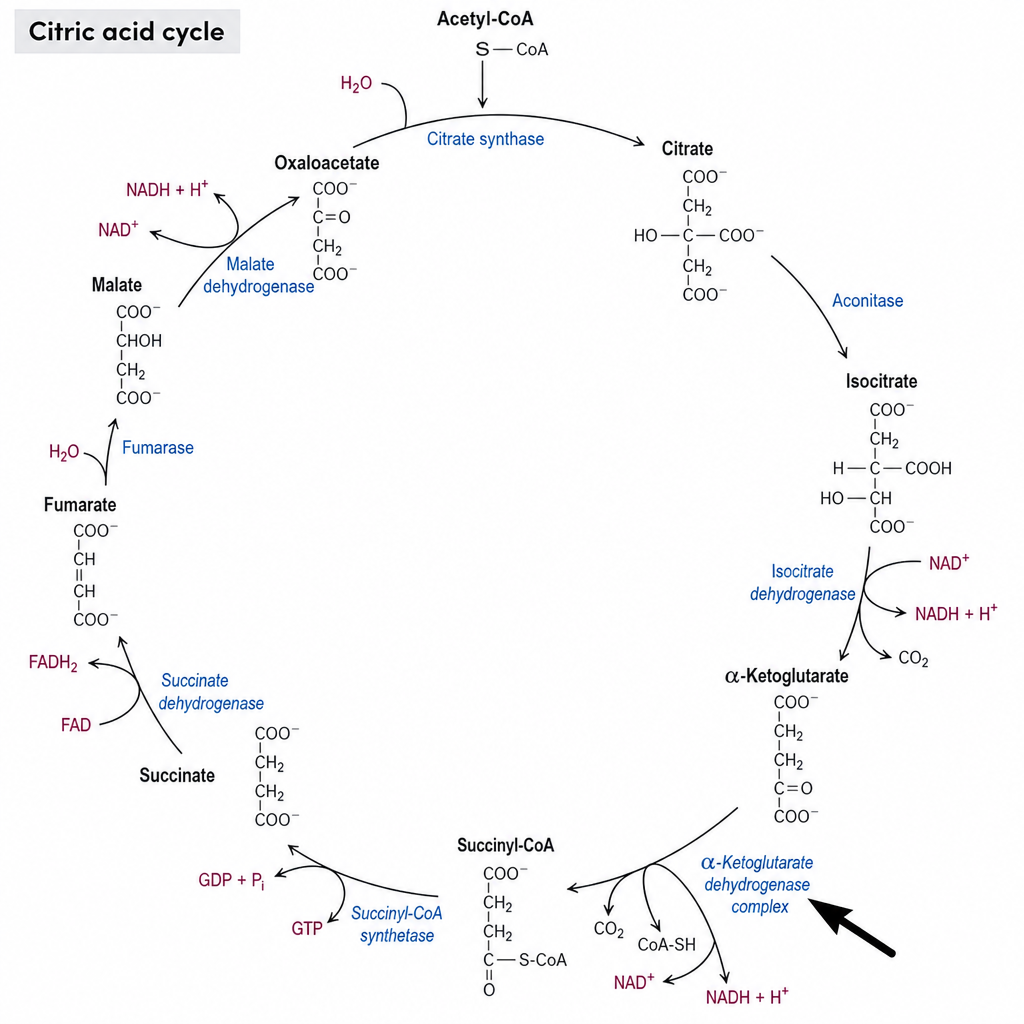
An investigator is studying the effect of extracellular pH changes on the substrates for the citric acid cycle. Which of the following vitamins is incorporated into the CoA substrate used in the reaction catalyzed by the enzyme marked by the arrow in the overview of the citric acid cycle?
A 70-year-old man with a long-standing history of diabetes mellitus type 2 and hypertension presents with complaints of constant wrist and shoulder pain. Currently, the patient undergoes hemodialysis 2 to 3 times a week and is on the transplant list for a kidney. The patient denies any recent traumas. Which of the following proteins is likely to be increased in his plasma, causing the patient’s late complaints?
A 4-day-old boy is brought to the physician by his mother because of vomiting, irritability, and poor feeding. Pregnancy and delivery were uncomplicated. Physical examination shows increased muscle tone in all extremities. He appears lethargic. His diapers emit a caramel-like odor. Urine studies are positive for ketone bodies. Supplementation of which of the following is most likely to improve this patient's condition?
A 20-year-old female presents to the college health clinic concerned about a rash that has recently developed along her back and flank. Aside from a history of chronic diarrhea and flatulence, she reports being otherwise healthy. She is concerned that this rash could be either from bed bugs or possibly be sexually transmitted, as she has engaged in unprotected sex multiple times over the past two years. The physician orders several lab tests and finds that the patient does indeed have chlamydia and elevated tissue transglutaminase (tTG) levels. What is the most likely cause of her rash?
A 55-year-old woman is brought to the physician by her daughter because of progressive memory loss and weakness over the past 6 months. She is now unable to perform activities of daily living and has had several falls in her apartment. She has diarrhea but has not had nausea or vomiting. She was treated for tuberculosis 10 years ago. She smoked half a pack of cigarettes daily for 25 years but stopped 8 years ago. She drinks a pint of vodka daily. Vital signs are within normal limits. Examination shows glossitis and a hyperpigmented rash on her face and arms. There are multiple bruises over both arms. On mental status examination, she is oriented to place and person only. Short-term memory is impaired; she can recall 0 out of 5 objects after 10 minutes. Which of the following deficiencies is most likely present in this patient?
You are counseling a mother whose newborn has just screened positive for a deficit of phenylalanine hydroxylase enzyme. You inform her that her child will require dietary supplementation of which of the following?
A 6-year-old girl is referred to the pediatrician after a primary care practitioner found her to be anemic, in addition to presenting with decreased bowel movements, intermittent abdominal pain, and hearing loss. The child has also shown poor performance at school and has lost interest in continuing her classes of glazed pottery that she has taken twice a week for the past year. During the examination, the pediatrician identifies gingival lines, generalized pallor, and moderate abdominal pain. Laboratory tests show elevated iron and ferritin concentration, and a blood smear shows small and hypochromic erythrocytes, basophilic stippling, and the presence of nucleated erythroblasts with granules visualized with Prussian blue. Which of the following molecules cannot be produced in the erythrocytes of this patient?
A 9-month-old boy is brought to the pediatrician because he cannot sit on his own without support and has involuntary movements. He was born vaginally with no complications at full term. There is no history of consanguinity among parents. On physical examination, it was noticed that he is a stunted infant with generalized hypotonia and severe generalized dystonic movements. The mother says that she has noticed the presence of orange sand in his diapers many times. Laboratory evaluation revealed elevated uric acid levels in both blood and urine. Which of the following enzymes is deficient in this patient?
A 25-year-old male visits his physician because of fertility issues with his wife. Physical exam reveals bilateral gynecomastia, elongated limbs, and shrunken testicles. Levels of plasma gonadotropins are elevated. Which of the following is also likely to be increased in this patient:
Practice by Chapter
TCA cycle reactions and regulation
Practice Questions
Electron transport chain and oxidative phosphorylation
Practice Questions
Pentose phosphate pathway
Practice Questions
Gluconeogenesis
Practice Questions
Glycogen metabolism
Practice Questions
Amino acid metabolism
Practice Questions
Integration of metabolic pathways
Practice Questions
Fed state vs. fasting state metabolism
Practice Questions
Exercise metabolism
Practice Questions
Alcohol metabolism
Practice Questions
Metabolic adaptations in starvation
Practice Questions
Metabolic disorders overview
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app