
Lipid metabolism — MCQs

On this page
A 14-year-old girl presents with her mother to a physician's office. They are both concerned with the amount of hair growing on the girl's upper lip and cheeks. There are also sparse hairs on her chest. The mother reports that her daughter has not started menstruating either. The girl was born at 39 weeks gestation via spontaneous vaginal delivery. She is up to date on all vaccines and is meeting all developmental milestones. On examination, the patient is in the 55th percentile for her height. Her blood pressure is 90/50 mm Hg, pulse is 75/min, and respirations are 15/min. There is thin dark hair on her upper lip and on her cheeks. She also has pustular acne on her face and shoulders. Her breasts are in the initial stages of development and she speaks with a deep voice describing her concerns to the physician. Based on her clinical history, which of the following enzymes are most likely deficient?
A 42-year-old man presents for evaluation of vitamin D deficiency with possible osteomalacia. The patient had a pathologic fracture 3 weeks ago and was found to have dangerously low levels of vitamin D with normal serum calcium levels. Bone density has been drastically affected, leading to the fracture this patient experienced. The lack of what compound is most responsible for the formation of this disease?
An 8-year-old boy is brought in for initial evaluation by a pediatrician after he was adopted from an international orphanage. On presentation, he is found to have difficulty with walking as well as bone and joint pain. The adoption papers for the child state that he was the product of a normal birth with no medical issues noted at that time. Since then, he has not seen a doctor until this presentation. Physical exam reveals bowed legs, hard lumps on his ribs, and tenderness to palpation over his bones. He is found to be low in a substance that directly promotes intestinal absorption of a nutrient. Which of the following is a characteristic of the substance that is abnormally low in this patient?
A 46-year-old man presents to the office complaining of dry, irritated eyes that have gotten worse over the last week. The patient states that he has also developed a red bumpy rash on his arms. On exam, his bilateral cornea and conjunctiva are dry and thickened. There are small ulcerations on the cornea. The skin of the bilateral arms has an erythematous rash characterized by small, white raised lesions. The patient has a history of alcoholism but has no other significant past medical history. What is most likely deficient in this patient?
A 53-year-old woman presents to her primary care doctor due to discolored, itchy skin, joint pain, and a feeling of abdominal fullness for the past week. Her medical history includes anxiety and depression. She also experiences occasional headaches and dizziness. Of note, the patient recently returned from an expedition to Alaska, where she and her group ate polar bear liver. Physical examination shows dry skin with evidence of excoriation and mild hepatosplenomegaly. Lab investigations reveal an alkaline phosphatase level of 35 U/L and total bilirubin of 0.4 mg/dL. Which of the following tests is most likely to uncover the etiology of her condition?
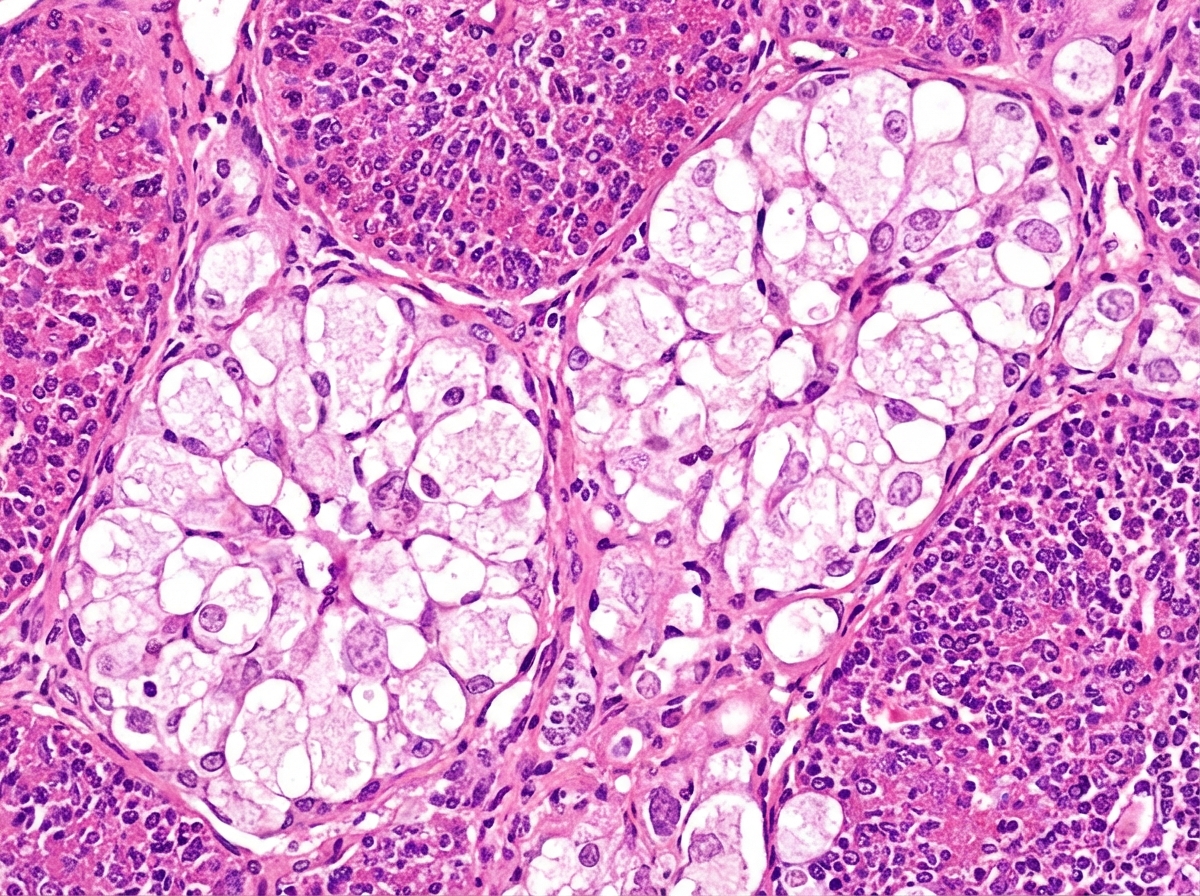
An 18-month-old boy is brought to the physician because of a 2-day history of cough, fever, and lethargy. He has been admitted to the hospital twice during the past year for pneumonia. He can stand without support but has not started to walk. He speaks in bisyllables. He is at the 3rd percentile for height and 4th percentile for weight. Examination shows diffuse crackles over bilateral lung fields. Abdominal examination shows hepatosplenomegaly. Fundoscopy shows bright red macular spots. Despite being given appropriate antibiotic therapy, the patient dies. A photomicrograph of a section of the spleen obtained during autopsy is shown. Accumulation of which of the following substances is the most likely cause of this patient's condition?
A 22-year-old man presents to the physician due to a progressively worsening weakness and an increasingly large abdomen. He notes that he eats well and is fairly active; however, his abdomen has become increasingly protuberant. He also complains of easy bruisability. His medical history is not significant and he takes no medications. Physical examination reveals hepatomegaly and splenomegaly. Several bruises can be seen on the inside of his arms and legs. His skin has a yellowish tinge to it. Laboratory testing shows the following: Hematocrit 25% Erythrocyte count 2.5 x 106/mm3 Thrombocyte count 25,000/mm3 A bone marrow biopsy shows a crinkled-paper appearance to the macrophages. Which of the following enzymes is most likely deficient in this patient?
A 57-year-old woman comes to the physician for a routine examination. She takes no medications. She swims 3 times weekly and jogs several miles with her dog on most mornings. Her diet consists primarily of vegetables, fish, and whole grains; she avoids processed foods and carbohydrates. She drinks one glass of red wine with dinner on most evenings. There is no family history of serious medical illness or cardiovascular disease. Physical examination shows no abnormalities. This patient is most likely to have an increase in which of the following laboratory markers?
A 12-year-old boy is brought to the emergency department with a hot, swollen, and painful knee. He was playing with his friends and accidentally bumped into one of them with his knee prior to presentation. His medical history is significant for an immunodeficiency syndrome, and he has been treated with long courses of antibiotics for multiple infections. His mother is concerned because he has also had significant bleeding that was hard to control following previous episodes of trauma. Laboratory tests are obtained with the following results: Prothrombin time: Prolonged Partial thromboplastin time: Prolonged Bleeding time: Normal The activity of which of the following circulating factors would most likely be affected by this patient's disorder?
A 19-year-old woman with a known history of malabsorption presents with a painful red tongue, red eyes, and cracked lips. She says her symptoms gradually began 4 months ago after moving away from home for college. She also complains of photophobia, spontaneous lacrimation, and itchy dermatitis. Past medical history is significant for a long-standing malabsorption syndrome, which she says that she hasn't been able to maintain her normal diet or take her vitamins regularly due to her busy schedule. The patient is afebrile and vital signs are within normal limits. On physical examination, she has a malnourished appearance with significant pallor. Conjunctival injection is present bilaterally. Which of the following diagnostic tests will be most helpful to support the diagnosis of the most likely vitamin deficiency in this patient?
Practice by Chapter
Fatty acid oxidation (beta-oxidation)
Practice Questions
Fatty acid synthesis
Practice Questions
Ketone body metabolism
Practice Questions
Cholesterol synthesis and regulation
Practice Questions
Lipoprotein metabolism
Practice Questions
Phospholipid metabolism
Practice Questions
Eicosanoid synthesis and function
Practice Questions
Steroid hormone synthesis
Practice Questions
Adipose tissue metabolism
Practice Questions
Brown vs. white adipose tissue
Practice Questions
Disorders of lipid metabolism
Practice Questions
Integration with carbohydrate metabolism
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app