
Lipid metabolism — MCQs

On this page
A patient with high triglycerides (TG) esterified with long-chain fatty acids (LCFA) presents with fatigue, and a biopsy of the muscle shows fat vacuoles. What is the most likely diagnosis?
A patient with tendon xanthomas, Increased LDL and cholesterol. What is the most probable diagnosis?
A previously healthy 8-year-old boy is brought to the physician because of increasing visual loss and deterioration of his hearing and speech over the past 2 months. During this period, he has had difficulty walking, using the stairs, and feeding himself. His teachers have noticed that he has had difficulty concentrating. His grades have worsened and his handwriting has become illegible. His maternal male cousin had similar complaints and died at the age of 6 years. Vital signs are within normal limits. Examination shows hyperpigmented skin and nails and an ataxic gait. His speech is dysarthric. Neurologic examination shows spasticity and decreased muscle strength in all extremities. Deep tendon reflexes are 4+ bilaterally. Plantar reflex shows an extensor response bilaterally. Sensation is decreased in the lower extremities. Fundoscopy shows optic atrophy. There is sensorineural hearing loss bilaterally. Which of the following is the most likely cause of this patient's symptoms?
The human body obtains vitamin D either from diet or from sun exposure. Darker-skinned individuals require more sunlight to create adequate vitamin D stores as the increased melanin in their skin acts like sunscreen; thus, it blocks the necessary UV required for vitamin D synthesis. Therefore, if these individuals spend inadequate time in the light, dietary sources of vitamin D are necessary. Which of the following requires sunlight for its formation?
A 25-year-old woman presents to you for a routine health checkup. She has no complaints. Family history is significant for 2 of her siblings who have died from Tay-Sachs disease, but she and her parents are phenotypically normal. Which of the following are the chances of this person being a heterozygous carrier of the mutation that causes Tay-Sachs disease?
A 7-year-old boy is brought to the pediatrician by his parents due to pubic hair growth and changes in his voice. He has been developing in the 98th percentile for his age. His vaccination is up-to-date. The patient’s blood pressure is within the 60th percentile for his age. Physical examination reveals pubic and armpit hair, and Tanner stage 2 characterized by enlarged scrotum and testes. Laboratory findings are significant for the following: Hemoglobin 13.1 g/dL Hematocrit 39.7% Leukocyte count 8,500/mm3 Neutrophils 65% Lymphocytes 30% Monocytes 5% Mean corpuscular volume 82.2 μm3 Platelet count 20,000/mm3 Urine creatinine clearance 98 mL/min Serum 17-hydroxyprogesterone 313 ng/dL (normal <110 ng/dL) Which of the following enzymes is most likely to be defective in this patient?
A 34-year-old woman with Crohn disease comes to the physician because of a 4-week history of nausea, bloating, and epigastric pain that occurs after meals and radiates to the right shoulder. Four months ago, she underwent ileocecal resection for an acute intestinal obstruction. An ultrasound of the abdomen shows multiple echogenic foci with acoustic shadows in the gallbladder. Which of the following mechanisms most likely contributed to this patient’s current presentation?
A 73-year-old woman is brought to the physician by her son because of a 2-month history of diarrhea and recurrent upper respiratory tract infections. Her son says that she frequently trips over the nightstand when she gets up to go to the bathroom at night. She is 173 cm (5 ft 8 in) tall and weighs 54 kg (120 lb); BMI is 18 kg/m2. Physical examination shows dry skin, multiple bruises on the shins, and triangular keratin plaques on the temporal half of the conjunctiva. A deficiency of which of the following is the most likely underlying cause of these findings?
A 35-year-old lactose intolerant man presents to the outpatient clinic with complaints of numbness and tingling in his fingers and toes for the past month. He also complains of pain in his calf muscles while sleeping; the pain is severe enough to wake him up in the middle of the night. He is a software engineer and spends most of his time indoors. He has been smoking a pack of cigarettes daily for the past 10 years and occasionally drinks wine with dinner. His current medication regimen includes as needed ibuprofen and calcium supplementation. He does not take any other multivitamins. On examination, his pulse rate is 74/min, blood pressure is 128/67 mm Hg, respiratory rate is 16/min, and temperature is 37.6°C (99.7°F). He has tenderness in the proximal muscles of his upper and lower limbs. Sensory examination is normal. The rest of the physical examination is normal. X-ray imaging of his lower limbs shows features of demineralization. Which of the following sets of abnormalities are most likely occurring in this patient?
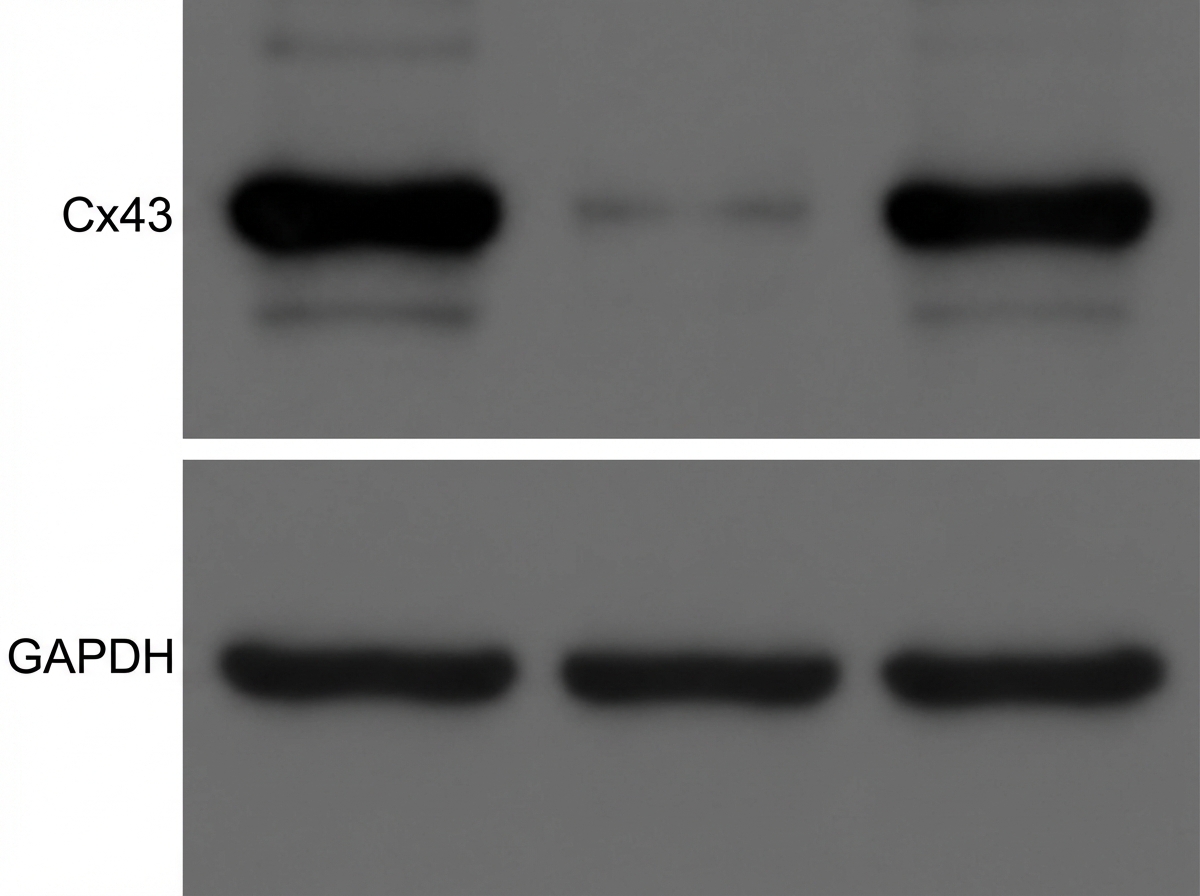
A researcher is investigating the relationship between inflammatory mediators and omega-3 fatty acids, namely docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA), in post-MI patients. IL-1ß is an important pro-inflammatory cytokine involved in fibrosis and arrhythmias in the post-MI period. Research indicates that it causes loss of function in the gap junction connexin 43 (Cx43), resulting in an arrhythmogenic state. They perform an experiment investigating the cardioprotective effect of DHA on patients after a recent MI. Their results are shown in a Western blot analysis. The Western blot contains three lanes labeled as follows: Lane 1 = Control, Lane 2 = IL-1β, Lane 3 = IL-1β + DHA. Which of the following is the most accurate conclusion from these results?
Practice by Chapter
Fatty acid oxidation (beta-oxidation)
Practice Questions
Fatty acid synthesis
Practice Questions
Ketone body metabolism
Practice Questions
Cholesterol synthesis and regulation
Practice Questions
Lipoprotein metabolism
Practice Questions
Phospholipid metabolism
Practice Questions
Eicosanoid synthesis and function
Practice Questions
Steroid hormone synthesis
Practice Questions
Adipose tissue metabolism
Practice Questions
Brown vs. white adipose tissue
Practice Questions
Disorders of lipid metabolism
Practice Questions
Integration with carbohydrate metabolism
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app