
Disorders of lipid metabolism — MCQs

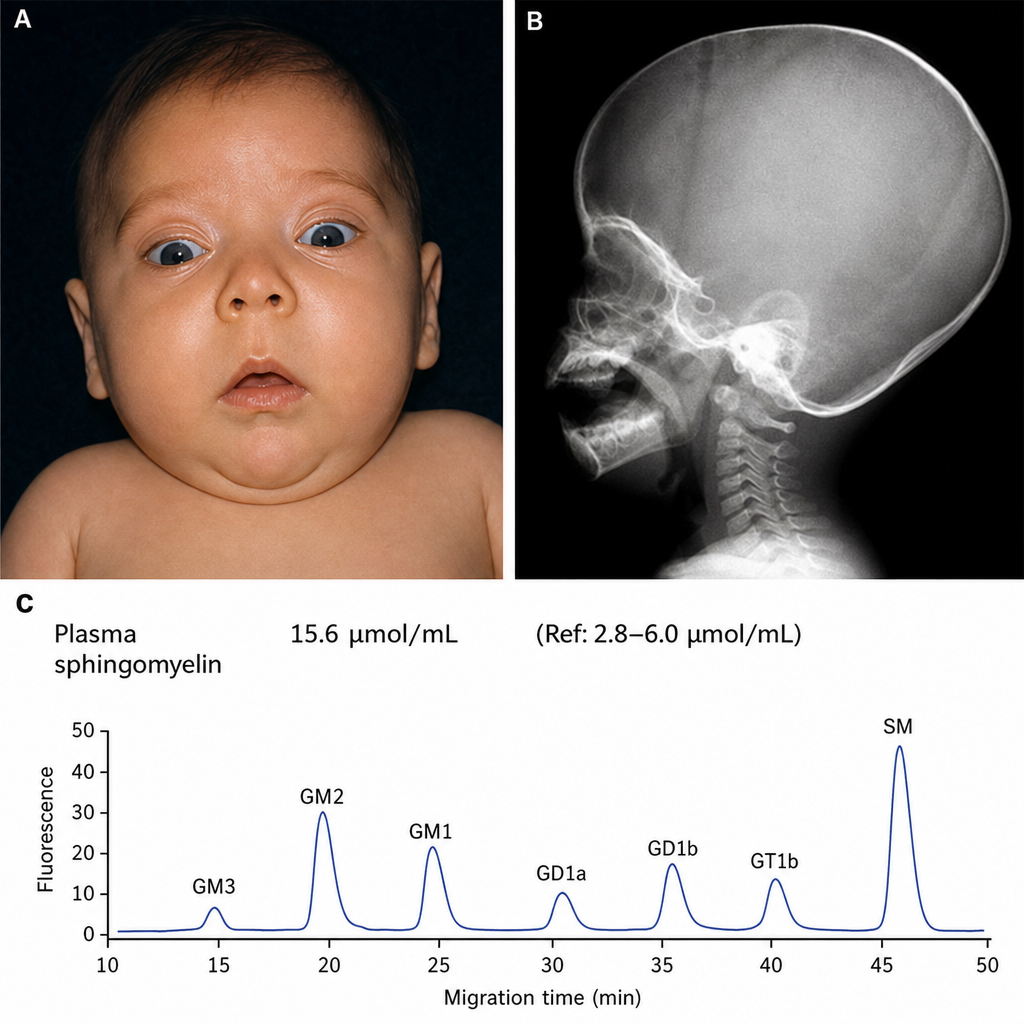
You examine an infant in your office. On exam you observe hypotonia, as well as the findings shown in Figures A and B. You order laboratory testing, which demonstrates the findings shown in Figure C. Which of the following is the most likely pathologic mechanism involved?
An 8-year-old boy presents to his primary care pediatrician for routine check-up. During the visit, his mom says that she has noticed yellow bumps on his eyelids and was concerned about whether they were a problem. Upon hearing this concern, the physician inquires about parental health history and learns that both parents have high cholesterol despite adhering to a statin regimen. Furthermore, other family members have suffered early myocardial infarctions in their 30s. Physical exam reveals flat yellow patches on the patient's eyelids bilaterally as well as hard yellow bumps around the patient's ankles. Based on clinical suspicion an LDL level is obtained and shows a level of 300 mg/dL. What protein is most likely defective in this patient causing these findings?
A previously healthy 22-year-old man comes to the physician because of multiple nodules on his hands that first appeared a few months ago. He works as a computer game programmer. His father died of a myocardial infarction at 37 years of age, and his mother has rheumatoid arthritis. A photograph of the lesions is shown. The nodules are firm, mobile, and nontender. Which of the following is the most likely mechanism underlying this patient's skin findings?

An 18-month-old boy of Ashkenazi-Jewish descent presents with loss of developmental milestones. On ocular exam, a cherry-red macular spot is observed. No hepatomegaly is observed on physical exam. Microscopic exam shows lysosomes with onion-skin appearance. What is the most likely underlying biochemical abnormality?
A 33-year-old man presents with his recent laboratory results. He has no symptoms currently, but he underwent a medical evaluation as a requirement for taking up a new job. His medical history is not significant. His laboratory reports are as follows: Blood hemoglobin 13.7 g/dL Leukocyte count 8,000/mm3 Platelet count 350,000/mm3 Serum creatinine 0.8 mg/dL Serum alanine aminotransferase 16 U/L Serum aspartate aminotransferase 14 U/L Serum cholesterol 450 mg/dL Serum triglyceride 790 mg/dL Serum LDL cholesterol 150 mg/dL Serum HDL cholesterol 55 mg/dL Which of the following findings is most likely to be present on physical examination of this patient?
A 57-year-old man presents for a regular check-up. He does not have any complaints at the time of presentation. He has a history of several episodes of acute non-necrotizing pancreatitis with the last episode being 2 years ago. Also, he was diagnosed with hypertension 5 years ago. Currently, he takes aspirin, atorvastatin, enalapril, and indapamide. He plays tennis twice a week, does low impact cardio workouts 3 times a week, and follows a low-fat diet. He smokes half a pack of cigarettes per day and refuses to quit smoking. The patient’s blood pressure is 140/85 mm Hg, heart rate is 88/min, respiratory rate is 14/min, and temperature is 36.6°C (97.9°F). His height is 181 cm (5 ft 11 in), weight is 99 kg (218 lb), and BMI is 30.8 kg/m2. Physical examination reveals multiple xanthomas on the patient’s trunk, elbows, and knees. Heart sounds are diminished with fixed splitting of S2 and an increased aortic component. The rest of the examination is unremarkable. The patient’s lipid profile shows the following results: Total serum cholesterol 235.9 mg/dL HDL 46.4 mg/dL LDL 166.3 mg/dL Triglycerides 600 mg/dL Glucose 99 mg/dL Which of the following modifications should be made to the patient’s therapy?
A 60-year-old patient is at his physician’s office for a routine health maintenance exam. The patient has a past medical history of osteoarthritis in his right knee and GERD that is well-controlled with over the counter medication. On a fasting lipid profile, he is found to have high cholesterol. The patient is started on daily atorvastatin to reduce his risk of cardiovascular disease. What is the major apolipoprotein found on the lipoprotein most directly affected by his statin medication?
A 35-year-old man comes to the physician because of fatigue and generalized weakness for the past year. He has noticed he has been having fewer bowel movements. He has had pain with defecation and small amounts of blood when wiping. He has not lost weight despite increased efforts to diet and exercise. He has had no fever, throat pain, or difficulty swallowing. His temperature is 36.5°C (97.7°F), pulse is 50/min, blood pressure is 120/90 mm Hg, and BMI is 35 kg/m2. Physical examination shows dry skin and a distended abdomen. There is 1+ pitting edema in the lower extremities. On neurological examination, deep tendon reflexes are 1+. Further evaluation of this patient is most likely to show which of the following findings?
A 12-year-old boy is brought to the physician because of difficulty in walking for 5 months. His mother reports that he has trouble keeping his balance and walking without support. Over the past year, he has started to have difficulty seeing in the dark and his hearing has been impaired. Examination shows marked scaling of the skin on the face and feet and a shortened 4th toe. Muscle strength is 3/5 in the lower extremities and 4/5 in the upper extremities. Sensation to pinprick is symmetrically decreased over the legs. Fundoscopy shows peripheral pigment deposits and retinal atrophy. His serum phytanic acid concentration is markedly elevated. The patient's condition is most likely caused by a defect in which of the following cellular structures?
Steroid hormone synthesis, lipid synthesis, and chemical detoxification are activities of which of the following?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app