
Study designs — MCQs

On this page
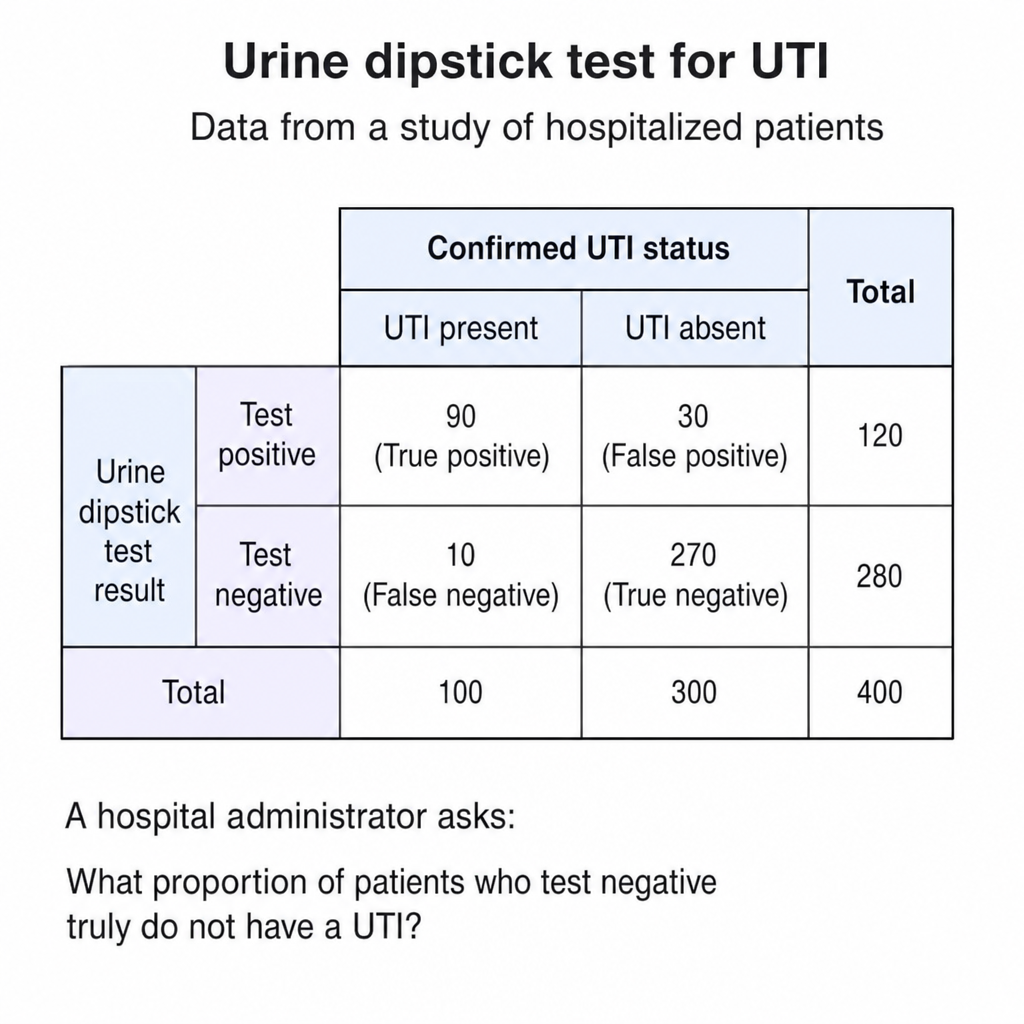
A researcher is reviewing data from a study evaluating a new urine dipstick test for detecting a urinary tract infection (UTI) in hospitalized patients. The following results were recorded: 90 patients with confirmed UTI tested positive, 10 with confirmed UTI tested negative, 30 patients without UTI tested positive, and 270 patients without UTI tested negative. A hospital administrator asks the researcher what proportion of patients who test negative truly do not have a UTI. Which value from the 2×2 table answers this question?
A research team has data from three completed studies on statin use and Alzheimer's disease: Study A (case-control, OR=0.6, n=500), Study B (retrospective cohort, RR=0.7, n=10,000), and Study C (RCT with cognitive decline as secondary endpoint, RR=0.9, n=2,000). The case-control study used prevalent cases, the cohort study had significant loss to follow-up in the unexposed group, and the RCT was underpowered for cognitive outcomes. Synthesize the evidence to determine the most reliable conclusion about the association.
A public health department needs to determine whether a cluster of birth defects in a county is associated with industrial pollution. They have limited resources, the suspected exposure occurred 3-5 years ago, and the outcome is rare (15 cases identified). Multiple potential confounders exist including maternal age, socioeconomic status, and prenatal care access. The community demands rapid answers. Evaluate the most appropriate initial study design considering feasibility, ethics, and scientific validity.
A pharmaceutical company wants to evaluate a new anticoagulant's effectiveness in preventing stroke in atrial fibrillation patients. They have limited funding and need results within 2 years. The drug has promising phase 2 data. Concurrent medications and comorbidities vary widely in the target population. The company must choose between a pragmatic trial in 50 community hospitals or an explanatory trial at 3 academic centers with strict protocols. Evaluate which design best serves both scientific and practical objectives.
A randomized controlled trial of a new diabetes medication shows significant reduction in HbA1c levels (p<0.001). However, 40% of participants in the treatment group and 15% in the placebo group dropped out before study completion, primarily due to gastrointestinal side effects in the treatment group. The analysis includes only participants who completed the study. Analyze the impact on study conclusions.
A study follows 5,000 healthcare workers from 1995 to 2015, tracking their exposure to bloodborne pathogens and development of chronic infections. The researchers use employment records to determine exposure history rather than relying on participant recall. In 2010, the hospital implemented a new electronic medical record system that improved documentation of needle-stick injuries. Analyze how this change affects the validity of the exposure assessment.
A researcher studies 300 patients with pancreatic cancer and 300 matched controls, collecting information about coffee consumption over their lifetime. The odds ratio for pancreatic cancer in heavy coffee drinkers is 3.2 (95% CI: 2.1-4.8). However, the researcher later discovers that cases were more likely to accurately recall their coffee intake because they had been contemplating possible causes of their illness. Analyze how this affects the study results.
A medical student conducts a study by surveying 800 adults at a community health fair about their current alcohol consumption and simultaneously measuring their liver enzyme levels. She finds that 15% of participants have elevated liver enzymes and 40% report heavy alcohol use. Apply your understanding to identify the primary limitation of this study design.
A physician researcher enrolls 2,000 healthy nurses aged 25-55 years and records their dietary habits, exercise patterns, and medication use. She plans to follow them for 20 years to determine who develops cardiovascular disease. Apply this information to determine what measure of association can be directly calculated from this study.
A pharmaceutical company conducts a study where 1,000 patients with hypertension are randomly assigned to receive either a new antihypertensive medication or placebo. Participants are followed for 5 years to assess the incidence of myocardial infarction. Neither the patients nor the investigators know who receives the active drug. Apply your knowledge to identify the key advantage of this study design.
Practice by Chapter
Observational studies vs experiments
Practice Questions
Cross-sectional studies
Practice Questions
Case-control studies
Practice Questions
Cohort studies
Practice Questions
Randomized controlled trials
Practice Questions
Meta-analyses and systematic reviews
Practice Questions
Qualitative research methods
Practice Questions
Survey design
Practice Questions
Sampling methods
Practice Questions
Blinding and controls
Practice Questions
Bias identification and mitigation
Practice Questions
Confounding variables
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app