
Upper/Lower Limb — MCQs

On this page
A 23-year-old female college basketball player presents in Sports Clinic after she felt a "pop" in her knee after coming down with a rebound. To examine the patient, you have her lie down on the table with her knees flexed 90 degrees. With your hand around her knee you are able to draw the tibia toward you from underneath the femur. The torn structure implicated by this physical exam maneuver has which of the following attachments?
A 68-year-old right hand-dominant man presents to the emergency room complaining of severe right arm pain after falling down a flight of stairs. He landed on his shoulder and developed immediate severe upper arm pain. Physical examination reveals a 2-cm laceration in the patient’s anterior right upper arm. Bone is visible through the laceration. An arm radiograph demonstrates a displaced comminuted fracture of the surgical neck of the humerus. Irrigation and debridement is performed immediately and the patient is scheduled to undergo definitive operative management of his fracture. In the operating room on the following day, the operation is more complicated than expected and the surgeon accidentally nicks a neurovascular structure piercing the coracobrachialis muscle. This patient would most likely develop a defect in which of the following?
A 13-year-old girl is brought to the physician by her father because of a 1-month history of pain in her right knee. She is a competitive volleyball player and has missed several games recently due to pain. Examination shows swelling distal to the right knee joint on the anterior surface of the proximal tibia; there is no overlying warmth or deformity. Extension of the right knee against resistance is painful. Which of the following structures is attached to the affected anterior tibial area?
A 37-year-old man is brought to the emergency department after being attacked with a knife. Physical examination shows a 4-cm laceration in the midline of the right forearm. An MRI of the right arm shows damage to a nerve that runs between the superficial and deep flexor digitorum muscles. Loss of sensation over which of the following areas is most likely in this patient?
A 3629-g (8-lb) newborn is examined shortly after spontaneous vaginal delivery. She was delivered at 40 weeks' gestation and pregnancy was uncomplicated. Her mother is concerned because she is not moving her left arm as much as her right arm. Physical examination shows her left arm to be adducted and internally rotated, with the forearm extended and pronated, and the wrist flexed. The Moro reflex is present on the right side but absent on the left side. Which of the following brachial plexus structures is most likely injured in this infant?
An 8-year-old boy is brought to the emergency department after falling from a trampoline and landing on his left arm. On presentation, he is found to be holding his left arm against his chest and says that his arm is extremely painful just above the elbow. Radiographs are obtained showing the finding in figure A. The boy's arm is reduced and placed into a splint pending surgical fixation. If this patient's fracture is associated with a nerve injury, which of the following actions would he most likely be unable to perform in the emergency department?

An 18-year-old man comes to the physician because of severe left shoulder pain after a basketball match. During the game, the patient sustained an injury to the posterior part of his outstretched arm after being blocked by a defender. Examination shows no gross deformity of the left shoulder. Palpation of the shoulder elicits mild tenderness. Internal rotation of the arm against resistance shows weakness. These findings are most specific for injury to which of the following muscles?
A 44-year-old woman comes to the physician for the evaluation of right knee pain for 1 week. The pain began after the patient twisted her knee during basketball practice. At the time of the injury, she felt a popping sensation and her knee became swollen over the next few hours. The pain is exacerbated by walking up or down stairs and worsens throughout the day. She also reports occasional locking of the knee. She has been taking acetaminophen during the past week, but the pain is worse today. Her mother has rheumatoid arthritis. The patient is 155 cm (4 ft 11 in) tall and weighs 75 kg (165 lb); BMI is 33 kg/m2. Vital signs are within normal limits. Examination shows effusion of the right knee; range of motion is limited by pain. There is medial joint line tenderness. Knee extension with rotation results in an audible snap. Further evaluation is most likely to show which of the following?
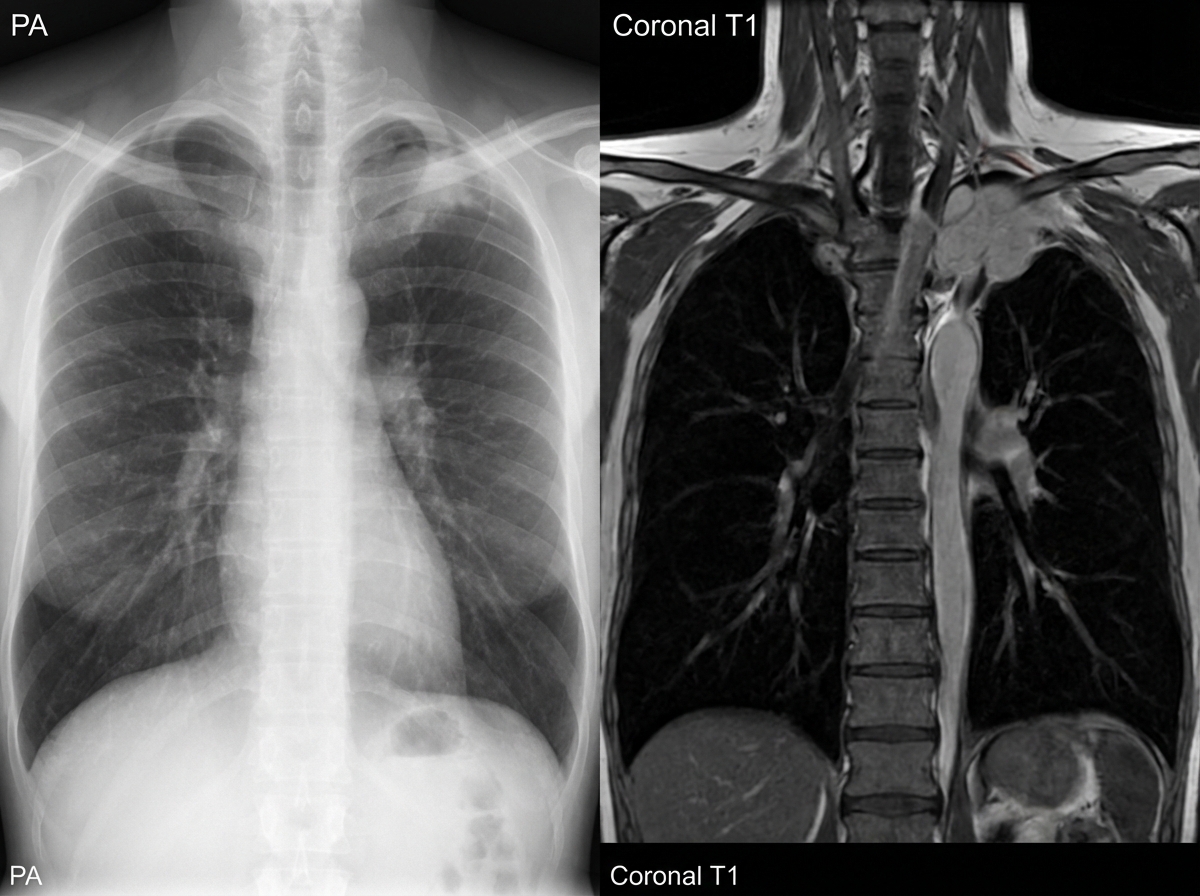
A 16-year-old girl presents with episodes of sharp pain in her left upper limb. She says her symptoms gradually onset a few months ago and have progressively worsened. She describes her pain as severe and feeling like "someone stabbing me in my arm and then the pain moves down to my hand". She says the pain is worse after physical activity and improves with rest. She also says she has some vision problems in her left eye. The patient is afebrile, and her vital signs are within normal limits. On physical examination, there are no visible deformities in the shoulders or upper extremities. Palpation of her left upper limb reveals tenderness mainly near her neck. Mild left-sided ptosis is present. There is anisocoria of her left pupil which measures 1 mm smaller than the right. The right upper limb is normal. A plain radiograph and an MRI are ordered (shown in the image). Which of the following focal neurologic deficits would most likely be seen on the left hand of this patient?
A 72-year-old woman presents with left lower limb swelling. She first noticed her left leg was swollen about 2 weeks ago. She denies any pain and initially thought the swelling would subside on its own. Past medical history is significant for hypertension and hyperlipidemia. She is a smoker with a 35 pack-year history and an occasional drinker. She takes chlorthalidone, lisinopril, atorvastatin and a multivitamin. On physical examination, her left leg appears larger than her right with 2+ pitting edema up to her knee. She also has a few distended superficial veins along the posterior aspect of her left leg. Lower extremities have 2+ pulses bilaterally. The ultrasound of her left lower thigh and leg shows an obstructing thrombosis of the distal portion of the femoral vein. Which of the following veins serve as collateral pathways to help mitigate the consequences of this patient's condition?
Practice by Chapter
Bones and joints of upper limb
Practice Questions
Muscles and movements of upper limb
Practice Questions
Nerves and blood supply of upper limb
Practice Questions
Clinical correlations of upper limb
Practice Questions
Bones and joints of lower limb
Practice Questions
Muscles and movements of lower limb
Practice Questions
Nerves and blood supply of lower limb
Practice Questions
Clinical correlations of lower limb
Practice Questions
Comparison of upper and lower limb structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app