
Upper/Lower Limb — MCQs

On this page
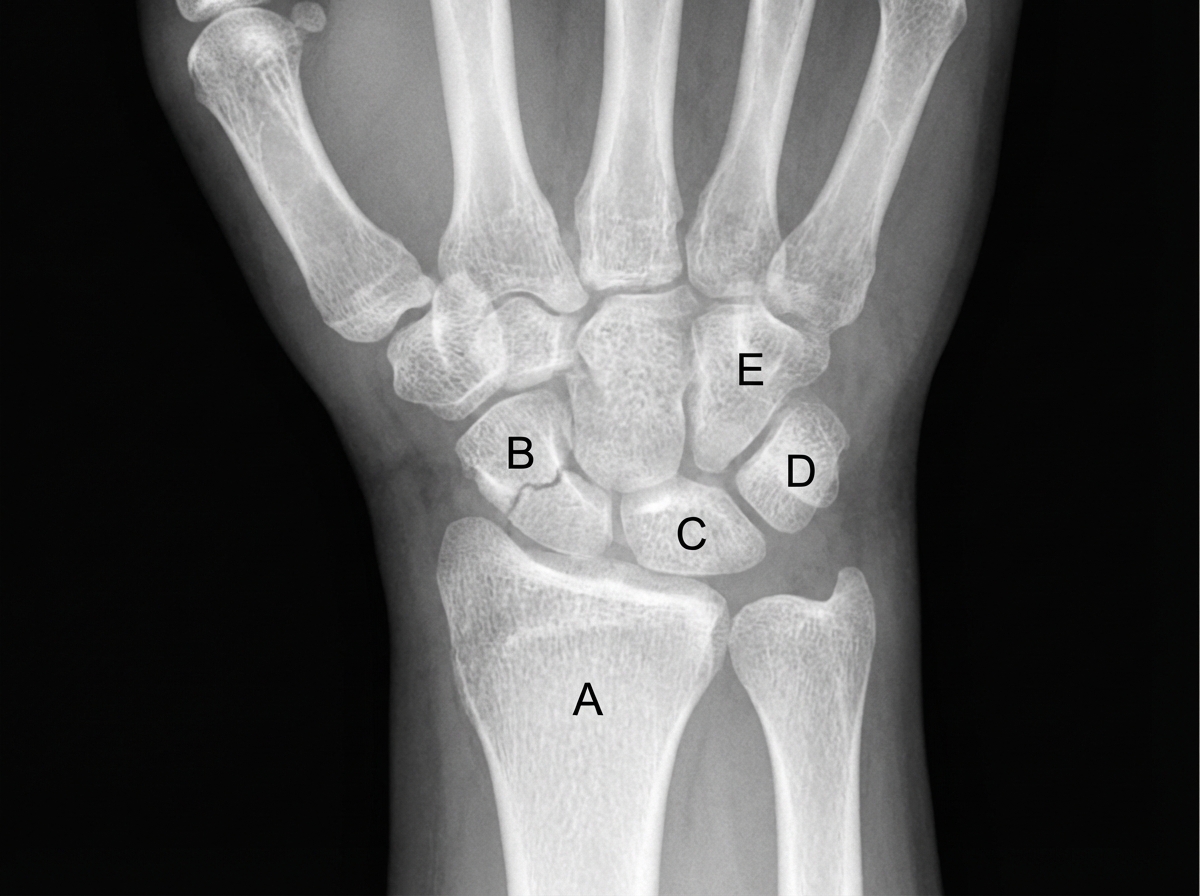
A 33-year-old woman presents to the emergency department with pain in her right wrist. She says she was walking on the sidewalk a few hours ago when she suddenly slipped and landed forcefully on her outstretched right hand with her palm facing down. The patient is afebrile, and vital signs are within normal limits. Physical examination of her right wrist shows mild edema and tenderness on the lateral side of the right hand with a decreased range of motion. There is point tenderness in the anatomic snuffbox. Sensation is intact. The patient is able to make a fist and OK sign with her right hand. Based on the clinical findings, which of the following bones is most likely fractured in this patient?
A 41-year-old woman comes to the doctor because of gradually progressive weakness in her right hand over the past few weeks. She goes to the gym to lift weights 5 times a week. With the dorsum of the right hand on a flat surface, the patient is unable to move her thumb to touch a pen held 2 cm above the interphalangeal joint of the thumb. An MRI of the right arm shows compression of a nerve that passes through the pronator teres muscle. Based on the examination findings, loss of innervation of which of the following muscles is most likely in this patient?
A 26-year-old woman comes to the physician because of painful paresthesias in her foot. Examination shows decreased sensation in the first interdigital space and a hallux valgus deformity. This patient's paresthesias are most likely caused by compression of which of the following nerves?
A newborn infant is born at 41 weeks gestation to a healthy G1P0 mother. The delivery was complicated by shoulder dystocia. The infant is in the 89th and 92nd percentiles for height and weight, respectively. The mother's past medical history is notable for diabetes mellitus and obesity. Immediately after birth, the child's temperature is 99°F (37.2°C), blood pressure is 90/50 mmHg, pulse is 120/min, and respirations are 24/min. The child demonstrates a strong cry and pink upper and lower extremities bilaterally. The left arm is adducted and internally rotated at the shoulder and extended at the elbow. Extension at the elbow and flexion and extension of the wrist appear to be intact in the left upper extremity. The right upper extremity appears to have normal strength and range of motion in all planes. Which of the following sets of nerves or nerve roots is most likely affected in this patient?
A 23-year-old college student was playing basketball when he fell directly onto his left elbow. He had sudden, intense pain and was unable to move his elbow. He was taken immediately to the emergency room by his teammates. He has no prior history of trauma or any chronic medical conditions. His blood pressure is 128/84 mm Hg, the heart rate is 92/min, and the respiratory rate is 14/min. He is in moderate distress and is holding onto his left elbow. On physical examination, pinprick sensation is absent in the left 5th digit and the medial aspect of the left 4th digit. Which of the following is the most likely etiology of this patient’s condition?
A newborn infant is born at 42 weeks gestation to a healthy 36-year-old G1P0. The delivery was complicated by prolonged labor and shoulder dystocia. The child is in the 87th and 91st percentiles for height and weight at birth, respectively. The mother’s past medical history is notable for diabetes mellitus and obesity. Immediately after birth, the child’s temperature is 99°F (37.2°C), blood pressure is 90/50 mmHg, pulse is 120/min, and respirations are 24/min. The child demonstrates a strong cry and pink upper and lower extremities bilaterally. The right arm is adducted and internally rotated at the shoulder and extended at the elbow. Flexion and extension of the wrist and digits appear to be intact in the right upper extremity. Which of the following muscles would most likely have normal strength in this patient?
A 31-year-old woman presents with difficulty walking and climbing stairs for the last 3 weeks. She has no history of trauma. The physical examination reveals a waddling gait with the trunk swaying from side-to-side towards the weight-bearing limb. When she stands on her right leg, the pelvis on the left side falls. When she stands on her left leg, the pelvis remains level. Which of the following nerves is most likely injured in this patient?
A 65-year-old man comes to a follow-up appointment with his surgeon 2 months after undergoing hip replacement surgery. His major concern at this visit is that he is still limping since the surgery even after the post-operative pain has subsided. Specifically, when he stands on his right leg, he feels that he has to lean further to the right in order to maintain balance. When standing on his left leg, he feels that he is able to step normally. Damage to which of the following nerves would most likely present with this patient's symptoms?
A 38-year-old man comes to the physician because of a 3-week history of right-sided knee pain. He works as a bricklayer and reports that the pain worsens when he kneels. He has no history of trauma. Examination of the right knee shows erythema, fluctuant swelling, and tenderness on palpation of the kneecap. Passive flexion of the right knee elicits pain. Which of the following structures is most likely affected in this patient?
A 12-year-old boy is brought to the physician because of a 6-day history of gradually worsening left knee pain. The pain is exacerbated by movement and kneeling. There is no pain at rest and no history of trauma to the knee. He is concerned because his soccer tryouts are in a few days. Vital signs are within normal limits. Examination shows mild swelling and tenderness to palpation of the left anterior, superior tibia. Extension of the left knee against resistance reproduces the knee pain; flexion is limited by pain. There is no local erythema or effusion of the left knee. A lateral view of an x-ray of his left knee is shown. Which of the following is the most likely underlying cause of this patient's symptoms?

Practice by Chapter
Bones and joints of upper limb
Practice Questions
Muscles and movements of upper limb
Practice Questions
Nerves and blood supply of upper limb
Practice Questions
Clinical correlations of upper limb
Practice Questions
Bones and joints of lower limb
Practice Questions
Muscles and movements of lower limb
Practice Questions
Nerves and blood supply of lower limb
Practice Questions
Clinical correlations of lower limb
Practice Questions
Comparison of upper and lower limb structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app