
Upper/Lower Limb — MCQs

On this page
A 12-year-old boy presents to the emergency department after falling from his bike. He is holding his right arm tenderly and complains of pain in his right wrist. When asked, he says that he fell after his front tire hit a rock and landed hard on his right hand. Upon physical examination he is found to have tenderness on the dorsal aspect of his wrist in between the extensor pollicis longus and the extensor pollicis brevis. Given this presentation, which of the following is the most likely bone to have been fractured?
A 36-year-old woman comes to the physician because of new onset limping. For the past 2 weeks, she has had a tendency to trip over her left foot unless she lifts her left leg higher while walking. She has not had any trauma to the leg. She works as a flight attendant and wears compression stockings to work. Her vital signs are within normal limits. Physical examination shows weakness of left foot dorsiflexion against minimal resistance. There is reduced sensation to light touch over the dorsum of the left foot, including the web space between the 1st and 2nd digit. Further evaluation is most likely to show which of the following?
A 16-year-old boy presents to the emergency room with severe right shoulder pain following a painful overhead swing during a competitive volleyball match. On physical examination, the patient has limited active range of motion of the right shoulder and significant pain with passive motion. Suspecting a rotator cuff injury, the physician obtains an MRI, which indicates a minor tear in the tendon of the rotator cuff muscle that is innervated by the axillary nerve. Which of the following muscles was affected?
A 35-year-old man is brought to the trauma bay by ambulance after sustaining a gunshot wound to the right arm. The patient is in excruciating pain and states that he can't move or feel his hand. The patient states that he has no other medical conditions. On exam, the patient's temperature is 98.4°F (36.9°C), blood pressure is 140/86 mmHg, pulse is 112/min, and respirations are 14/min. The patient is alert and his Glasgow coma scale is 15. On exam, he has a single wound on his right forearm without continued bleeding. The patient has preserved motor and sensation in his right elbow; however, he is unable to extend his wrist or extend his fingers further. He is able to clench his hand, but this is limited by pain. On sensory exam, the patient has no sensation to the first dorsal web space but has preserved sensation on most of the volar surface. Which of the following structures is most likely injured?
A 27-year-old female ultramarathon runner presents to the physician with complaints of persistent knee pain. She describes the pain to be located in the anterior area of her knee and is most aggravated when she performs steep descents down mountains, though the pain is present with running on flat roads, walking up and down stairs, and squatting. Which of the following would most likely be an additional finding in this patient’s physical examination?
A 57-year-old man presents to the ED complaining of back and left leg pain. He was lifting heavy furniture while helping his daughter move into college when all of sudden he felt a sharp pain at his back. The pain is described as severe, worse with movement, and shoots down his lateral thigh. The patient denies any bowel/urinary incontinence, saddle anesthesia, weight loss, or weakness. He denies any past medical history but endorses a family history of osteoporosis. He has been smoking 1 pack per day for the past 20 years. Physical examination demonstrated decreased sensation at the left knee, decreased patellar reflex, and a positive straight leg test. There is diffuse tenderness to palpation at the lower back but no vertebral step-offs were detected. What is the most likely etiology for this patient’s pain?
A 46-year-old man is brought to the emergency department for the onset of severe pain in his right knee that occurred when he tripped while descending a staircase. As he landed, he heard and felt an immediate popping sensation in his right knee. His medical history is positive for obesity, hypertension, type 2 diabetes mellitus, severe asthma, and hyperlipidemia. He currently takes lisinopril, hydrochlorothiazide, metformin, atorvastatin, an albuterol inhaler, and a fluticasone inhaler. He recently completed a hospitalization and week-long regimen of systemic corticosteroids for a severe exacerbation of his asthma. The patient's family history is not significant. In the emergency department, his vital signs are normal. On physical examination, his right knee is warm and swollen and he rates the pain as 9/10. He cannot stand or walk due to pain. He is unable to extend his right knee. A knee X-ray is ordered. Which of the following would best describe the cause of this presenting condition?
An 80-year-old woman is brought to the emergency department for left hip pain 30 minutes after she fell while walking around in her room. Examination shows left groin tenderness. The range of motion of the left hip is limited because of pain. An x-ray of the hip shows a linear fracture of the left femoral neck with slight posterior displacement of the femur. Which of the following arteries was most likely damaged in the patient's fall?
A 32-year-old man comes to the physician because of a 1-month history of intermittent tingling of his hand. He is an avid cyclist and has recently started training for a cycle marathon. Physical examination shows decreased grip strength in the right hand and wasting of the hypothenar eminence. On asking the patient to grasp a piece of paper between his right thumb and right index finger in the first web space, there is hyperflexion of the right thumb interphalangeal joint. Which of the following additional findings is most likely in this patient?
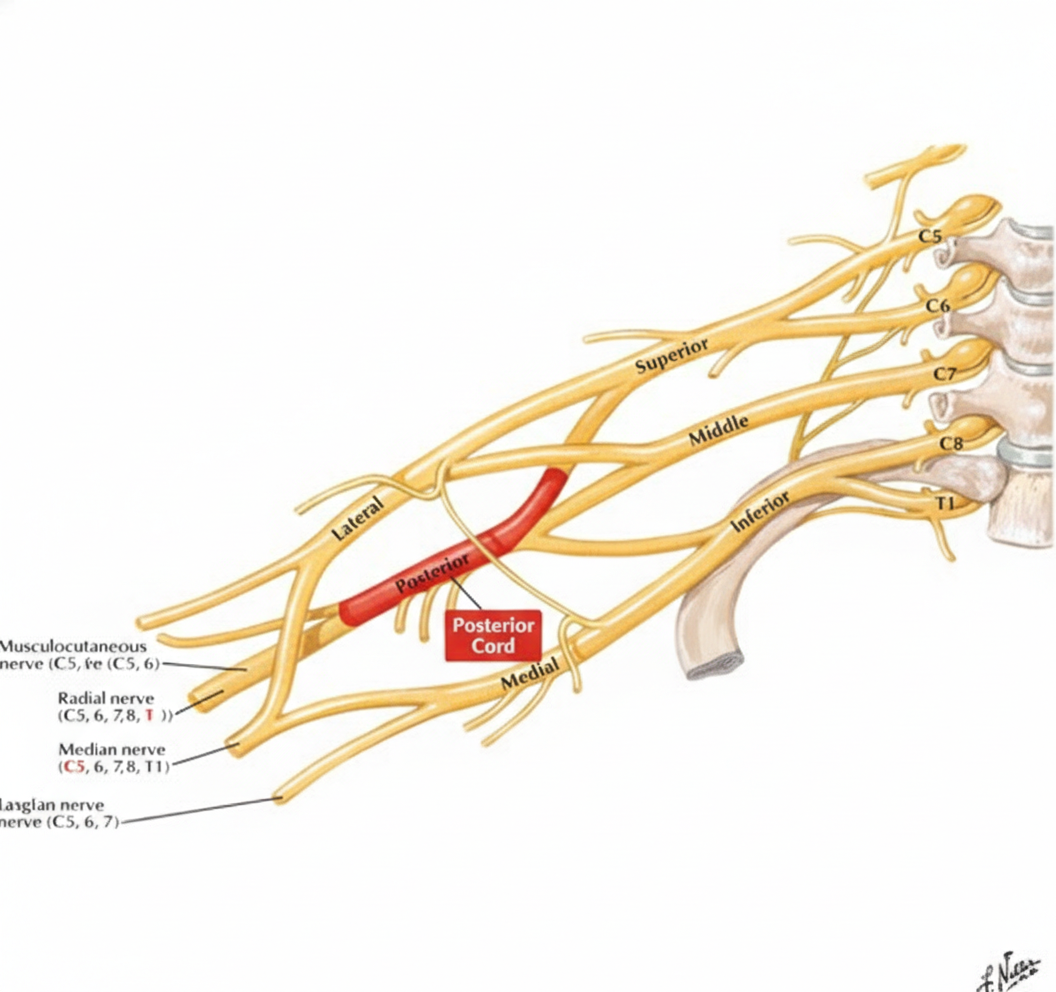
A 43-year-old woman comes to the physician because of tingling and weakness in her left arm for the past 2 days. An image of the brachial plexus is shown. Nerve conduction study shows decreased transmission of electrical impulses in the labeled structure. Physical examination is most likely to show impairment of which of the following movements?
Practice by Chapter
Bones and joints of upper limb
Practice Questions
Muscles and movements of upper limb
Practice Questions
Nerves and blood supply of upper limb
Practice Questions
Clinical correlations of upper limb
Practice Questions
Bones and joints of lower limb
Practice Questions
Muscles and movements of lower limb
Practice Questions
Nerves and blood supply of lower limb
Practice Questions
Clinical correlations of lower limb
Practice Questions
Comparison of upper and lower limb structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app