
Upper/Lower Limb — MCQs

On this page
A 17-year-old boy comes to the physician because of a 3-month history of pain in his right shoulder. He reports that he has stopped playing for his high school football team because of persistent difficulty lifting his right arm. Physical examination shows impaired active abduction of the right arm from 0 to 15 degrees. After passive abduction of the right arm to 15 degrees, the patient is able to raise his arm above his head. The dysfunctional muscle in this patient is most likely to be innervated by which of the following nerves?
A 28-year-old man comes to the physician because of a 3-month history of pain in his left shoulder. He is physically active and plays baseball twice a week. The pain is reproduced when the shoulder is externally rotated against resistance. Injury of which of the following tendons is most likely in this patient?
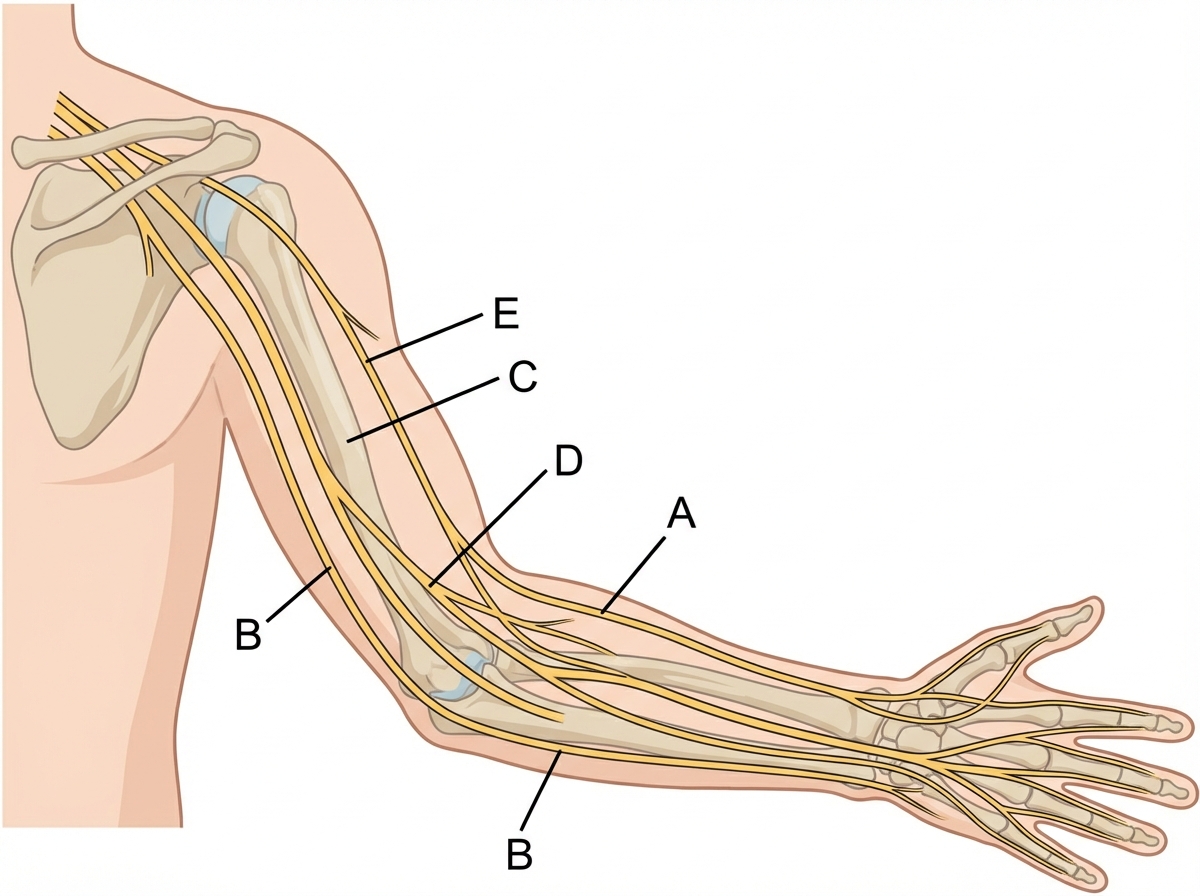
A 52-year-old female with a history of poorly-controlled diabetes presents to her primary care physician because of pain and tingling in her hands. These symptoms began several months ago and have been getting worse such that they interfere with her work as a secretary. She says that the pain is worse in the morning and she has been woken up at night by the pain. The tingling sensations have been located primarily in the thumb, index and middle fingers. On physical exam atrophy of the thenar eminence is observed and the pain is reproduced when the wrist is maximally flexed. The most likely cause of this patient's symptoms affects which of the nerves shown in the image provided?
A 34-year-old man is brought to the emergency department 3 hours after being bitten by a rattlesnake. He was hiking in the Arizona desert when he accidentally stepped on the snake and it bit his right leg. His pulse is 135/min and blood pressure is 104/81 mm Hg. Examination shows right lower leg swelling, ecchymosis, and blistering. Right ankle dorsiflexion elicits severe pain. A manometer inserted in the lateral compartment of the lower leg shows an intracompartmental pressure of 67 mm Hg. In addition to administration of the antivenom, the patient undergoes fasciotomy. Two weeks later, he reports difficulty in walking. Neurologic examination shows a loss of sensation over the lower part of the lateral side of the right leg and the dorsum of the right foot. Right foot eversion is 1/5. There is no weakness in dorsiflexion. Which of the following nerves is most likely injured in this patient?
A 51-year-old woman comes to the physician because of progressively worsening lower back pain. The pain radiates down the right leg to the lateral side of the foot. She has had no trauma, urinary incontinence, or fever. An MRI of the lumbar spine shows disc degeneration and herniation at the level of L5–S1. Which of the following is the most likely finding on physical examination?
A 10-year-old boy is referred to a pediatric neurologist by his pediatrician for lower extremity weakness. The boy is healthy with no past medical history, but his parents began to notice that he was having difficulty at football practice the previous day. Over the course of the past 24 hours, the boy has become increasingly clumsy and has been “tripping over himself.” On further questioning, the boy had a viral illness the previous week and was out of school for 2 days. Today, the patient’s temperature is 99.3°F (37.4°C), blood pressure is 108/72 mmHg, pulse is 88/min, respirations are 12/min. On motor exam, the patient has 5/5 strength in hip flexion, 5/5 strength in knee extension and flexion, 3/5 strength in foot dorsiflexion, and 5/5 strength in foot plantarflexion. The findings are the same bilaterally. On gait exam, the patient exhibits foot drop in both feet. Which of the following areas would the patient most likely have diminished sensation?
An 18-year-old man comes to the clinic with his mom for “pins and needles” of both of his arms. He denies any past medical history besides a recent anterior cruciate ligament (ACL) tear that was repaired 1 week ago. The patient reports that the paresthesias are mostly located along the posterior forearms, left more than the right. What physical examination finding would you expect from this patient?
Practice by Chapter
Bones and joints of upper limb
Practice Questions
Muscles and movements of upper limb
Practice Questions
Nerves and blood supply of upper limb
Practice Questions
Clinical correlations of upper limb
Practice Questions
Bones and joints of lower limb
Practice Questions
Muscles and movements of lower limb
Practice Questions
Nerves and blood supply of lower limb
Practice Questions
Clinical correlations of lower limb
Practice Questions
Comparison of upper and lower limb structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app