
Upper/Lower Limb — MCQs

On this page
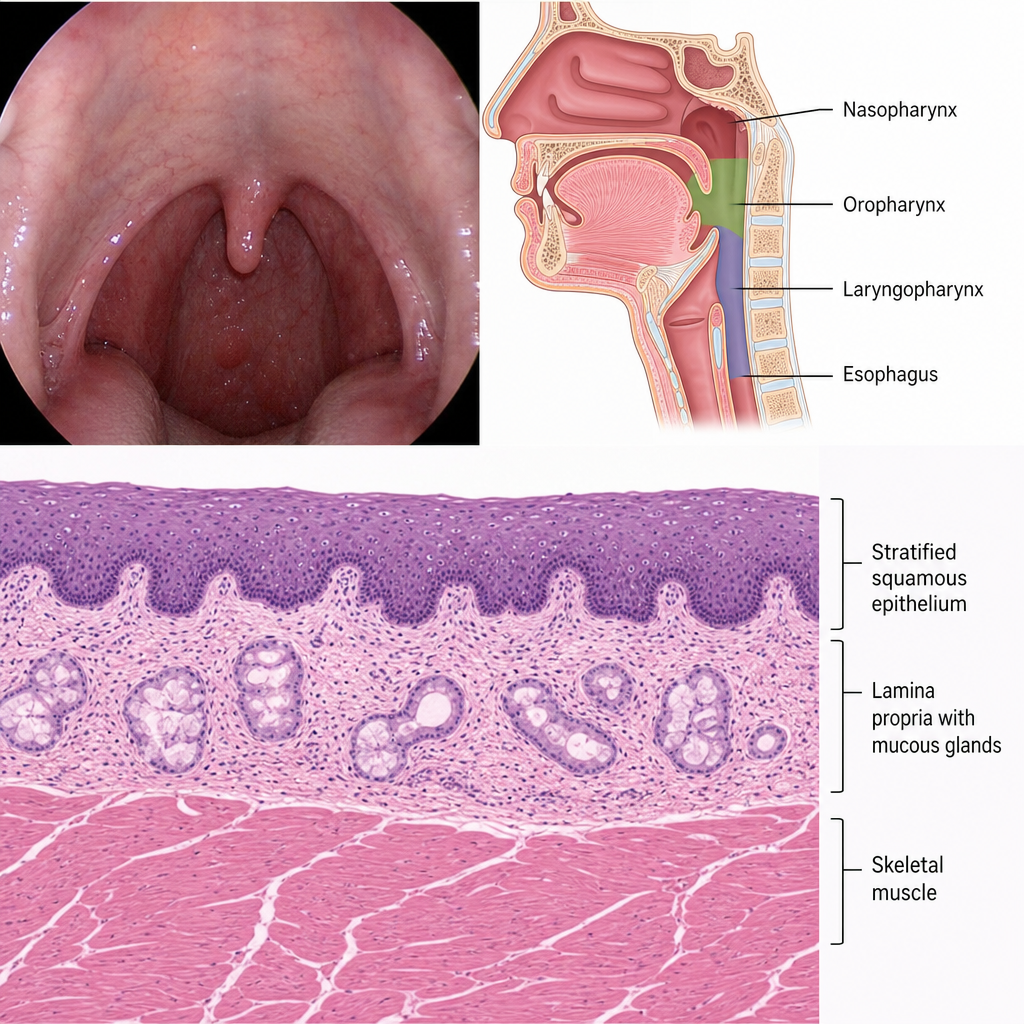
A biopsy of the posterior wall of the pharynx reveals a stratified squamous epithelium overlying a lamina propria rich in mucous glands, with underlying skeletal muscle. A student is asked to identify the embryological origin of the epithelial lining in this region. Which of the following correctly identifies the embryologic origin of this epithelium?
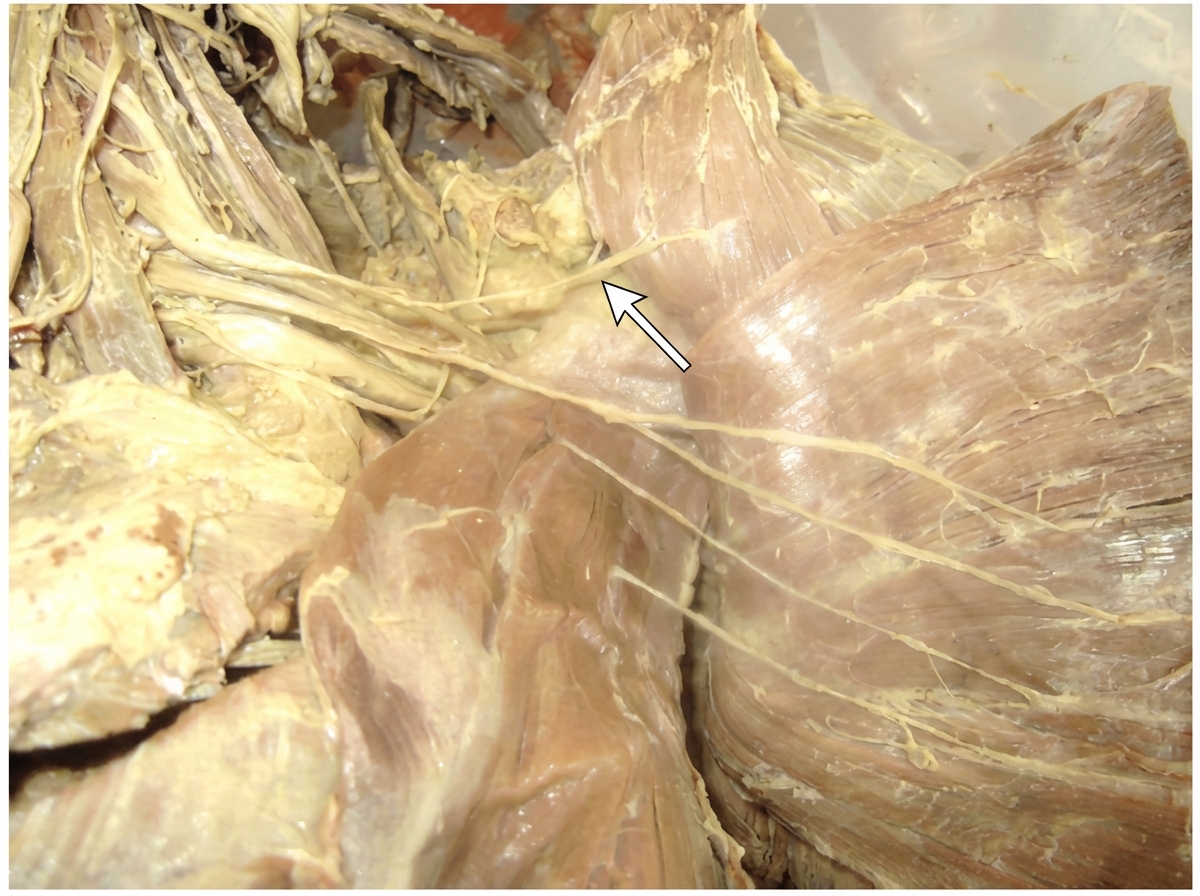
Identify the arrow marked nerve
A patient with a nerve injury was asked to form an "O" with their index finger and thumb but was unable to do so. Which muscle is most likely affected?
A patient diagnosed with sciatica has tender hamstrings. Which of the following nerves supplies a hybrid muscle that is partially spared in this patient?
Which artery is palpated behind the medial malleolus and in front of the Achilles tendon?
Practice by Chapter
Bones and joints of upper limb
Practice Questions
Muscles and movements of upper limb
Practice Questions
Nerves and blood supply of upper limb
Practice Questions
Clinical correlations of upper limb
Practice Questions
Bones and joints of lower limb
Practice Questions
Muscles and movements of lower limb
Practice Questions
Nerves and blood supply of lower limb
Practice Questions
Clinical correlations of lower limb
Practice Questions
Comparison of upper and lower limb structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app