
Thorax/Abdomen — MCQs

On this page
A researcher is investigating the blood supply of the adrenal gland. While performing an autopsy on a patient who died from unrelated causes, he identifies a vessel that supplies oxygenated blood to the inferior aspect of the right adrenal gland. Which of the following vessels most likely gave rise to the vessel in question?
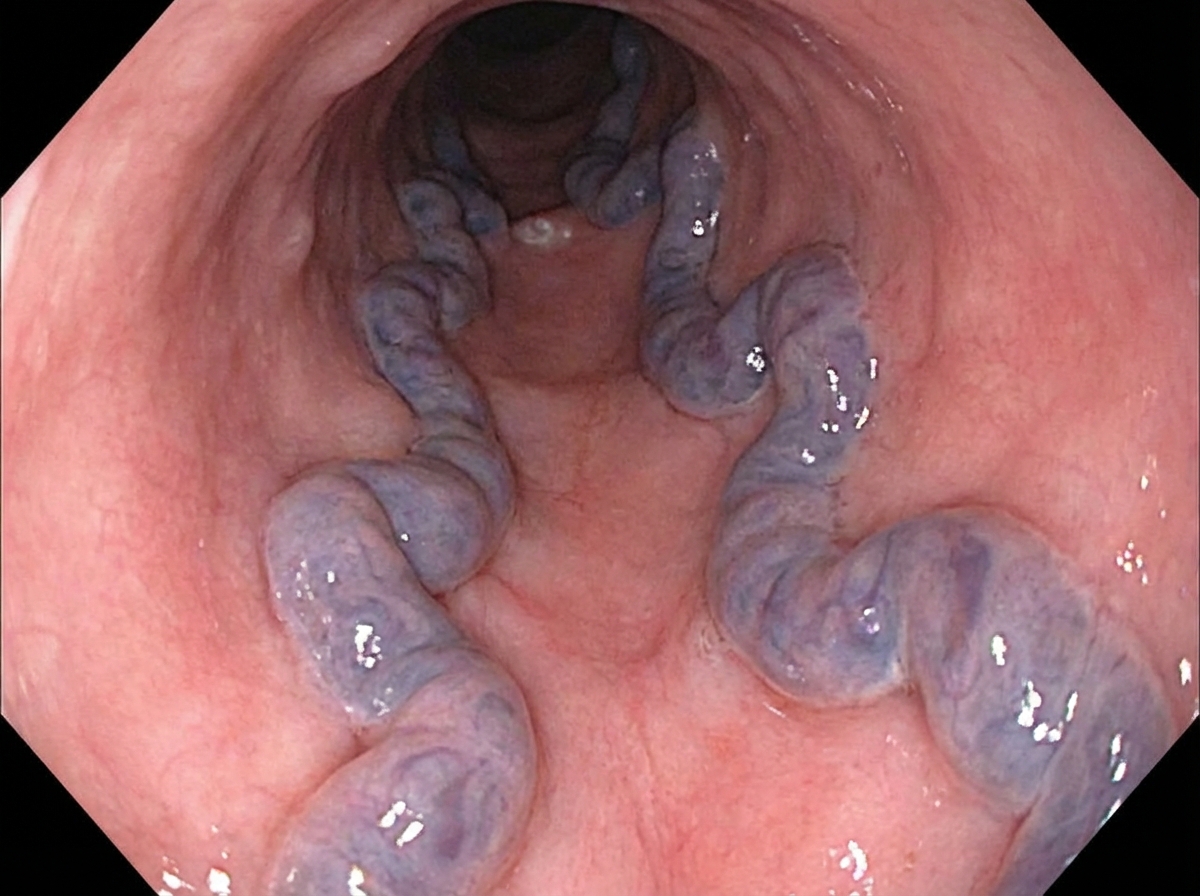
A 55-year-old man is brought to the emergency department by his friends after he was found vomiting copious amounts of blood. According to his friends, he is a chronic alcoholic and lost his family and job because of his drinking. The admission vital signs were as follows: blood pressure is 100/75 mm Hg, heart rate is 95/min, respiratory rate is 15/min, and oxygen saturation is 97% on room air. He is otherwise alert and oriented to time, place, and person. The patient was stabilized with intravenous fluids and a nasogastric tube was inserted. He is urgently prepared for endoscopic evaluation. An image from the procedure is shown. Which of the following vascular pairings corresponds specifically to the pathology shown on this patient's endoscopy?
A 45-year-old bank manager presents to the emergency department with abdominal pain for the last 2 weeks. The patient also vomited a few times, and in the last hour, he vomited blood as well. His pain was mild in the beginning but now he describes the pain as 8/10 in intensity, stabbing, and relentless. Ingestion of food makes it better as does the consumption of milk. He has a heart rate of 115/min. His blood pressure is 85/66 mm Hg standing, and 96/83 mm Hg lying down. He appears pale and feels dizzy. An intravenous line is started and a bolus of fluids is administered, which improved his vital signs. After stabilization, an esophagogastroduodenoscopy (EGD) is performed. There is a fair amount of blood in the stomach but after it is washed away, there are no abnormalities. A bleeding duodenal ulcer is seen located on the posteromedial wall of the duodenal bulb. Which artery is at risk from this ulcer?
A 65-year-old woman with atrial fibrillation comes to the emergency department because of sudden-onset severe abdominal pain, nausea, and vomiting for the past 2 hours. She has smoked a pack of cigarettes daily for the past 25 years. Her pulse is 110/min and blood pressure is 141/98 mm Hg. Abdominal examination shows diffuse abdominal tenderness without guarding or rebound. A CT angiogram of the abdomen confirms an acute occlusion in the inferior mesenteric artery. Which of the following structures of the gastrointestinal tract is most likely to be affected in this patient?
A 2-year-old girl is brought to the emergency department by her mother because the girl has had a cough and shortness of breath for the past 2 hours. Her symptoms began shortly after she was left unattended while eating watermelon. She appears anxious and mildly distressed. Examination shows intercostal retractions and unilateral diminished breath sounds with inspiratory wheezing. Flexible bronchoscopy is most likely to show a foreign body in which of the following locations?
A 45-year-old male is brought to the emergency department by emergency medical services after sustaining a gunshot wound to the abdomen. He is unresponsive. His temperature is 99.0°F (37.2°C), blood pressure is 95/58 mmHg, pulse is 115/min, and respirations are 20/min. Physical examination reveals an entry wound in the left abdominal quadrant just inferior to the left lateral costal border. Abdominal CT shows the bullet trajectory through the left abdominal cavity. Which of the following structures has the bullet most likely penetrated?
A 42-year-old woman presents to the emergency department complaining of abdominal pain, nausea, and vomiting for the last 4 hours. She says that symptoms onset right after she had 2 generous portions of pizza. She notes that she had prior similar episodes which resolved spontaneously within an hour. However, the pain today has persisted for 5 hours and is much more severe. She says the pain is located in the right upper quadrant of her abdomen and radiates to her upper back. She describes the pain as dull and cramping. She has had hypertension for the past 10 years, managed medically. Her vital signs are a blood pressure of 148/96 mm Hg, a pulse of 108/min, a respiratory rate of 18/min, and a temperature of 37.7°C (99.9°F). Her BMI is 28 kg/m2. On physical examination, the patient appears uncomfortable and is clutching her abdomen in pain. Abdominal exam reveals severe tenderness to palpation in the right upper quadrant with guarding. A positive Murphy’s sign is present. Her serum chemistry levels, including amylase, lipase, bilirubin, and liver function tests and urinalysis are normal. Urine hCG level is < 0.5 IU/L. Abdominal ultrasound reveals a large stone lodged in the neck of the gallbladder. Which of the following is the most likely pathway for referred pain in this patient?
A 68-year-old man with atrial fibrillation comes to the emergency department with acute-onset severe upper abdominal pain. He takes no medications. He is severely hypotensive. Despite maximal resuscitation efforts, he dies. Autopsy shows necrosis of the proximal portion of the greater curvature of the stomach caused by an embolic occlusion of an artery. The embolus most likely passed through which of the following vessels?
A 63-year-old man comes to the physician because of a 1-month history of difficulty swallowing, low-grade fever, and weight loss. He has smoked one pack of cigarettes daily for 30 years. An esophagogastroduodenoscopy shows an esophageal mass just distal to the upper esophageal sphincter. Histological examination confirms the diagnosis of locally invasive squamous cell carcinoma. A surgical resection is planned. Which of the following structures is at greatest risk for injury during this procedure?
A 68-year-old man comes to the physician because of a 4-month history of difficulty swallowing. During this time, he has also had a 7-kg (15-lb) weight loss. Esophagogastroduodenoscopy shows an exophytic mass in the distal third of the esophagus. Histological examination of a biopsy specimen shows a well-differentiated adenocarcinoma. The patient is scheduled for surgical resection of the tumor. During the procedure, the surgeon damages a structure that passes through the diaphragm along with the esophagus at the level of the tenth thoracic vertebra (T10). Which of the following structures was most likely damaged?
Practice by Chapter
Thoracic wall and diaphragm
Practice Questions
Pleura and lungs
Practice Questions
Mediastinum and heart
Practice Questions
Great vessels and lymphatics
Practice Questions
Abdominal wall and inguinal region
Practice Questions
Peritoneum and peritoneal cavity
Practice Questions
GI tract anatomy (esophagus to rectum)
Practice Questions
Liver, gallbladder and biliary tree
Practice Questions
Spleen and pancreas
Practice Questions
Kidneys and suprarenal glands
Practice Questions
Retroperitoneal structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app