
GI tract anatomy (esophagus to rectum) — MCQs

During a surgical procedure to repair an abdominal aortic aneurysm, the surgeon must be careful to avoid injury to which of the following arterial structures that originates near the level of the renal vessels?
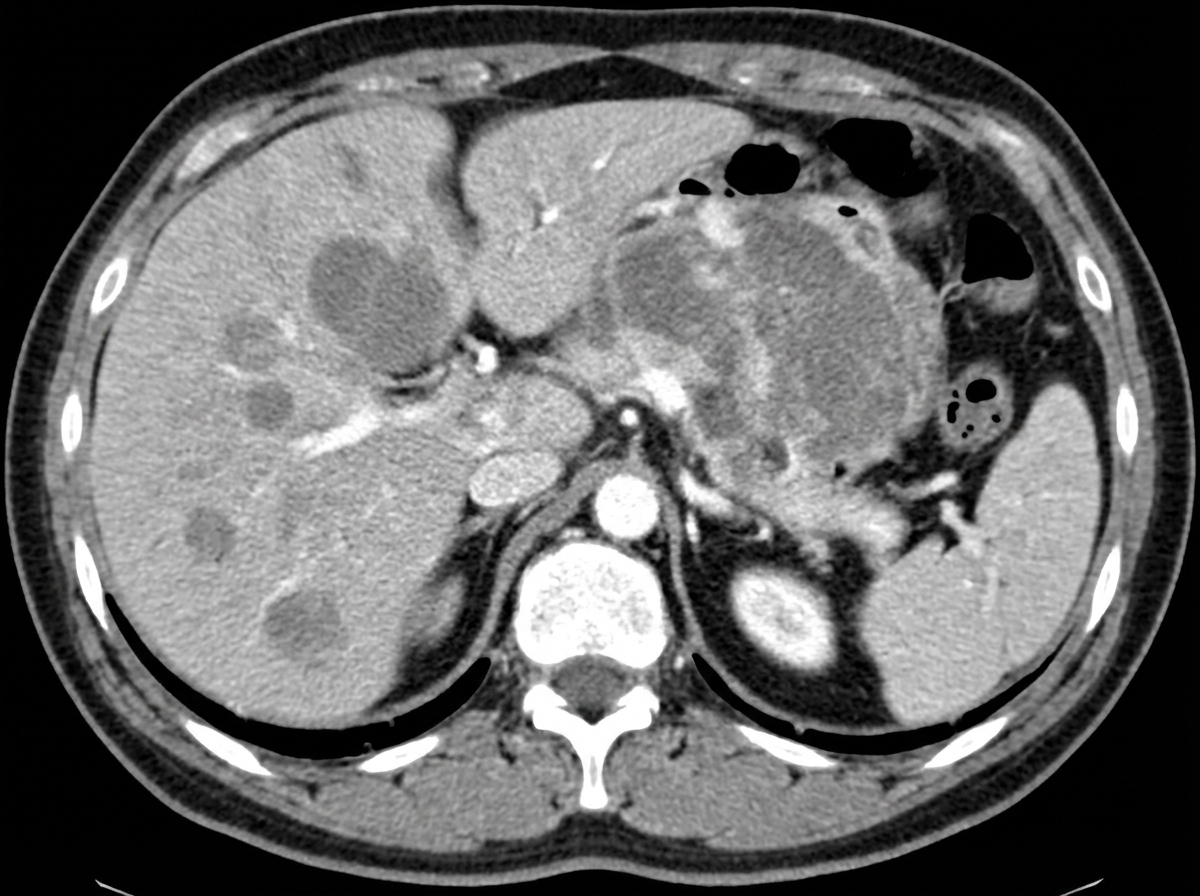
A 40-year-old man presents with severe fatigue, dyspnea on exertion, and weight loss. He reports a weight loss of 15 kg (33.0 lb) over the past 3 months and feels full almost immediately after starting to eat, often feeling nauseous and occasionally vomiting. Past medical history is not significant. However, the patient reports a 10-pack-year smoking history. His temperature is 37.0°C (98.6°F), respiratory rate is 15/min, pulse is 67/min, and blood pressure is 122/98 mm Hg. Physical examination reveals paleness and conjunctival pallor. Abdominal examination reveals an ill-defined nontender mass in the epigastric region along with significant hepatomegaly. Routine laboratory studies show a hemoglobin level of 7.2 g/dL. A contrast CT scan of the abdomen is presented below. Which of the following structures is most helpful in the anatomical classification of gastrointestinal bleeding in this patient?
A 69-year-old man presents with progressive dysphagia and a 5-kg weight loss over 3 months. Initially, he had difficulty swallowing solids, which progressed to include liquids in the past week. Endoscopy reveals a mass 3 cm proximal to the esophagogastric junction. Biopsy shows significant distortion of glandular architecture, consistent with adenocarcinoma. Which of the following is the strongest risk factor for this patient's likely diagnosis?
A 24-year-old woman comes to the emergency department because of abdominal pain, fever, nausea, and vomiting for 12 hours. Her abdominal pain was initially dull and diffuse but has progressed to a sharp pain on the lower right side. Two years ago she had to undergo right salpingo-oophorectomy after an ectopic pregnancy. Her temperature is 38.7°C (101.7°F). Physical examination shows severe right lower quadrant tenderness with rebound tenderness; bowel sounds are decreased. Laboratory studies show leukocytosis with left shift. An abdominal CT scan shows a distended, edematous appendix. The patient is taken to the operating room for an appendectomy. During the surgery, the adhesions from the patient's previous surgery make it difficult for the resident physician to identify the appendix. Her attending mentions that she should use a certain structure for guidance to locate the appendix. The attending is most likely referring to which of the following structures?
A 75-year-old man presents to the clinic for chronic fatigue of 3 months duration. Past medical history is significant for type 2 diabetes and hypertension, both of which are controlled with medications, as well as constipation. He denies any fever, weight loss, pain, or focal neurologic deficits. A complete blood count reveals microcytic anemia, and a stool guaiac test is positive for blood. He is subsequently evaluated with a colonoscopy. The physician notes some “small pouches” in the colon despite poor visualization due to inadequate bowel prep. What is the blood vessel that supplies the area with the above findings?
A 65-year-old woman with atrial fibrillation comes to the emergency department because of sudden-onset severe abdominal pain, nausea, and vomiting for the past 2 hours. She has smoked a pack of cigarettes daily for the past 25 years. Her pulse is 110/min and blood pressure is 141/98 mm Hg. Abdominal examination shows diffuse abdominal tenderness without guarding or rebound. A CT angiogram of the abdomen confirms an acute occlusion in the inferior mesenteric artery. Which of the following structures of the gastrointestinal tract is most likely to be affected in this patient?
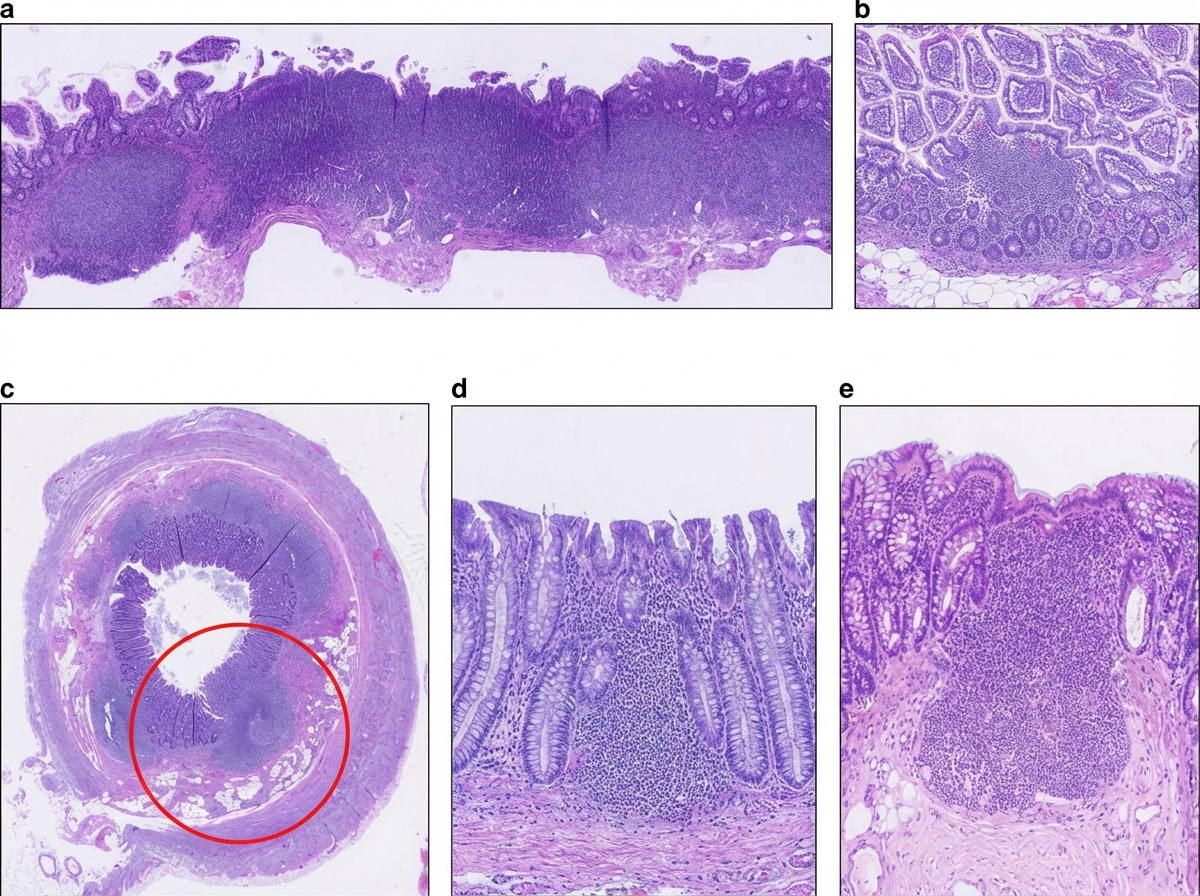
A 36-year-old man undergoes ileocecal resection after a gunshot injury. The resected ileocecal segment is sent for histological evaluation. One of the slides derived from the specimen is shown in the image. Which of the following statements regarding the structure marked within the red circle is correct?
A researcher is investigating the blood supply of the adrenal gland. While performing an autopsy on a patient who died from unrelated causes, he identifies a vessel that supplies oxygenated blood to the inferior aspect of the right adrenal gland. Which of the following vessels most likely gave rise to the vessel in question?
A 48-year-old Caucasian woman presents to her primary care provider complaining about difficulties while swallowing with fatigability and occasional palpitations for the past few weeks. Her personal history is relevant for bariatric surgery a year ago and a long list of allergies which includes peanuts, penicillin, and milk protein. Physical examination is unremarkable except for pale skin and mucosal surfaces, koilonychia, and glossitis. Which of the following descriptions would you expect to find in an endoscopy?
A 72-year-old male with a past medical history significant for aortic stenosis and hypertension presents to the emergency department complaining of weakness for the past 3 weeks. He states that, apart from feeling weaker, he also has noted lightheadedness, pallor, and blood-streaked stools. The patient's vital signs are stable, and he is in no acute distress. Laboratory workup reveals that the patient is anemic. Fecal occult blood test is positive for bleeding. EGD was performed and did not reveal upper GI bleeding. Suspecting a lower GI bleed, a colonoscopy is performed after prepping the patient, and it is unremarkable. What would be an appropriate next step for localizing a lower GI bleed in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app