
Thorax/Abdomen — MCQs

On this page
What is the most common site of congenital diaphragmatic hernia?
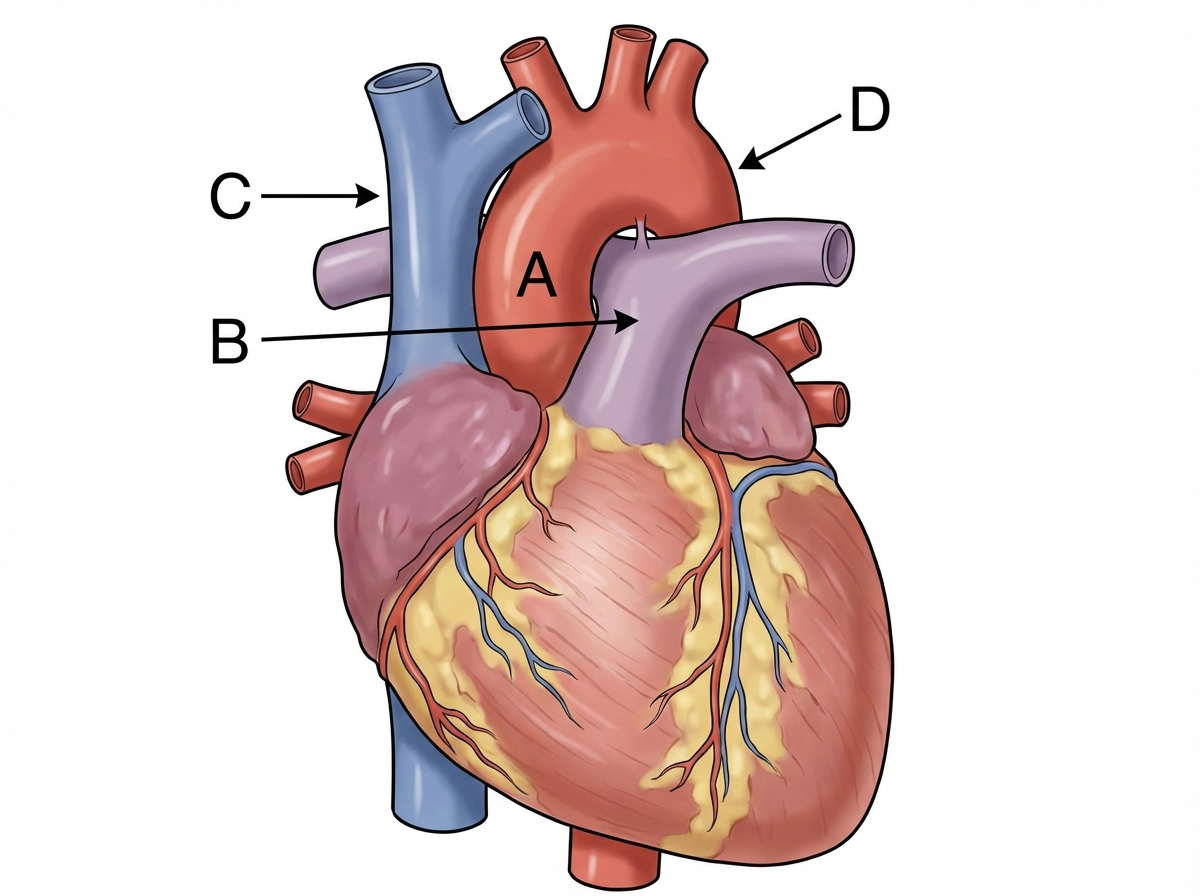
Identify the labeling correctly 
Structure preventing vertical descent of spleen
A 46-year-old male presents in consultation for weight loss surgery. He is 6’0” and weighs 300 pounds. He has tried multiple dietary and exercise regimens but has been unsuccessful in losing weight. The surgeon suggests a sleeve gastrectomy, a procedure that reduces the size of the stomach removing a large portion of the stomach along the middle part of the greater curvature. The surgeon anticipates having to ligate a portion of the arterial supply to this part of the stomach in order to complete the resection. Which of the following vessels gives rise to the vessel that will need to be ligated in order to complete the resection?
A 54-year-old woman comes to the physician because of a 3-month history of upper midthoracic back pain. The pain is severe, dull in quality, and worse during the night. Ten months ago, she underwent a modified radical mastectomy for invasive ductal carcinoma of the right breast. Physical examination shows normal muscle strength. Deep tendon reflexes are 2+ in all extremities. Examination of the back shows tenderness over the thoracic spinous processes. An x-ray of the thoracic spine shows vertebral osteolytic lesions at the levels of T4 and T5. The patient's thoracic lesions are most likely a result of metastatic spread via which of the following structures?
A 35-year-old obese man presents to the office complaining of chronic heartburn and nausea for the past 6 months. These symptoms are relieved when he takes 20 mg of omeprazole twice a day. The patient was prompted to come to the doctor when he recently experienced difficulty breathing and shortness of breath, symptoms which he believes underlies a serious health condition. The patient has no cardiac history but is concerned because his father recently died of a heart attack. Imaging of the patient’s chest and abdomen would most likely reveal which of the following?
A 75-year-old man presents to the clinic for chronic fatigue of 3 months duration. Past medical history is significant for type 2 diabetes and hypertension, both of which are controlled with medications, as well as constipation. He denies any fever, weight loss, pain, or focal neurologic deficits. A complete blood count reveals microcytic anemia, and a stool guaiac test is positive for blood. He is subsequently evaluated with a colonoscopy. The physician notes some “small pouches” in the colon despite poor visualization due to inadequate bowel prep. What is the blood vessel that supplies the area with the above findings?
An 18-year-old man is brought to the emergency department 30 minutes after being stabbed in the chest during a fight. He has no other injuries. His pulse is 120/min, blood pressure is 90/60 mm Hg, and respirations are 22/min. Examination shows a 4-cm deep, straight stab wound in the 4th intercostal space 2 cm medial to the right midclavicular line. The knife most likely passed through which of the following structures?
An 8-year-old boy is brought to the emergency department because of shortness of breath and dry cough for 2 days. His symptoms began after he helped his father clean the basement. He is allergic to shellfish. Respirations are 26/min. Physical examination shows diffuse end-expiratory wheezing and decreased inspiratory-to-expiratory ratio. This patient's symptoms are most likely being caused by inflammation of which of the following structures?
A 24-year-old man presents to the emergency room with a stab wound to the left chest at the sternocostal junction at the 4th intercostal space. The patient is hemodynamically unstable, and the trauma attending is concerned that there is penetrating trauma to the heart. Which cardiovascular structure is most likely to be injured first in this stab wound?
Practice by Chapter
Thoracic wall and diaphragm
Practice Questions
Pleura and lungs
Practice Questions
Mediastinum and heart
Practice Questions
Great vessels and lymphatics
Practice Questions
Abdominal wall and inguinal region
Practice Questions
Peritoneum and peritoneal cavity
Practice Questions
GI tract anatomy (esophagus to rectum)
Practice Questions
Liver, gallbladder and biliary tree
Practice Questions
Spleen and pancreas
Practice Questions
Kidneys and suprarenal glands
Practice Questions
Retroperitoneal structures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app