
Radiologic landmarks — MCQs

On this page
A 73-year-old man comes to the physician because of worsening bilateral lower extremity pain for the past 8 months. The pain begins after walking one to two blocks and radiates bilaterally down the buttocks with cramping and tingling. He reports that the pain is worse while walking downhill and is relieved by sitting and leaning forward. He has hypertension, hyperlipidemia, and type 2 diabetes mellitus. He had a myocardial infarction at the age of 55 years and an abdominal aortic aneurysm repair at the age of 60 years. He has smoked one pack of cigarettes daily for the past 30 years. He does not drink alcohol or use illicit drugs. His current medications include sitagliptin, metformin, atorvastatin, metoprolol succinate, amlodipine, and hydrochlorothiazide. His temperature is 37.5°C (99.5°F), pulse is 82/min, respirations are 17/min, and blood pressure is 150/87 mm Hg. Examination shows full muscle strength. Sensation is reduced bilaterally in the feet and toes. Straight leg raise is negative. X-ray of the spine shows degenerative changes. Which of the following is the most appropriate next step in diagnosis?
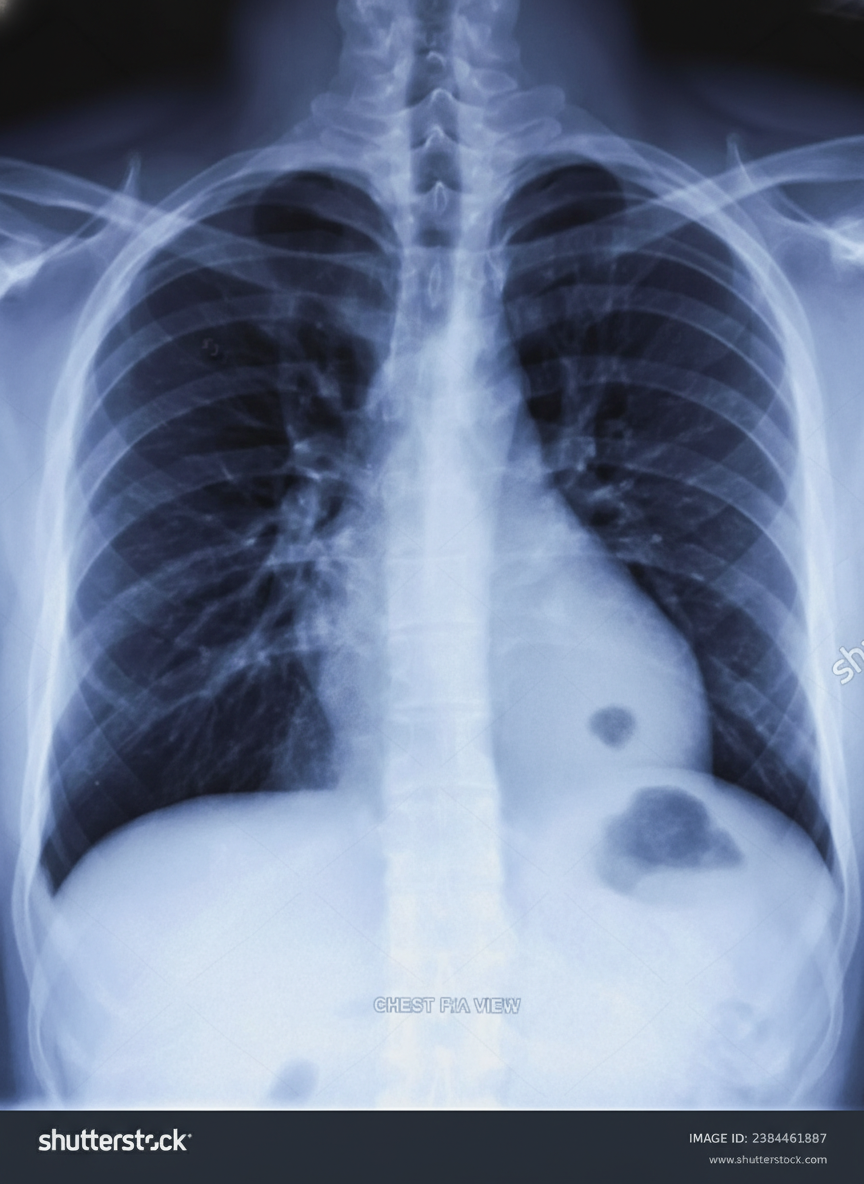
A 45-year-old man presents for a follow-up visit as part of his immigration requirements into the United States. Earlier this week, he was administered the Mantoux tuberculin skin test (TST). Today’s reading, 3 days after being administered the test, he shows an induration of 10 mm. Given his recent immigration from a country with a high prevalence of tuberculosis, he is requested to obtain a radiograph of the chest, which is shown in the image. Which of the following is true regarding this patient’s chest radiograph (CXR)?
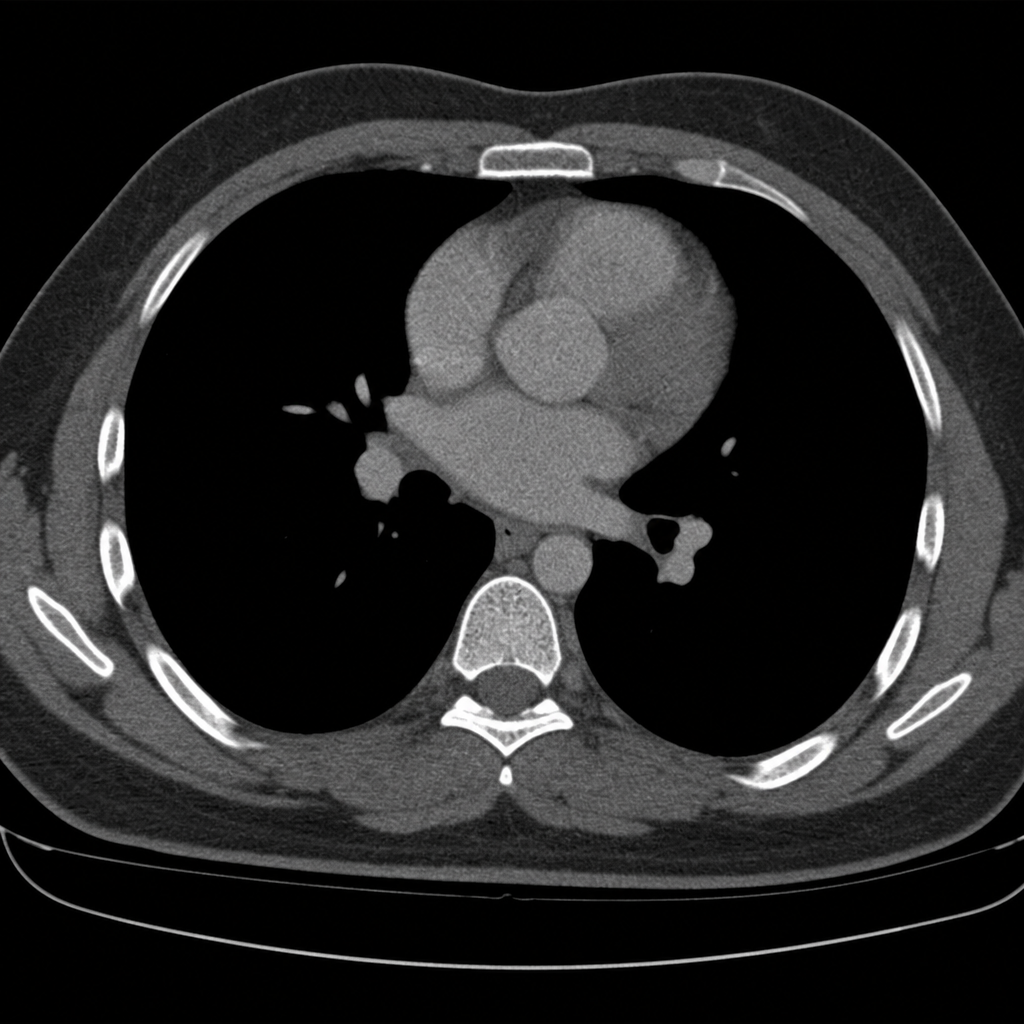
A 40-year-old woman is brought to the emergency department by a paramedic team from the scene of a motor vehicle accident where she was the driver. The patient was restrained by a seat belt and was unconscious at the scene. On physical examination, the patient appears to have multiple injuries involving the trunk and extremities. There are no penetrating injuries to the chest. As part of her trauma workup, a CT scan of the chest is ordered. Based on the mediastinal structures visible in this image, which approximate vertebral level does this image represent?
A 74-year-old male is brought to the emergency department 1 hour after he fell from the top of the staircase at home. He reports pain in his neck as well as weakness of his upper extremities. He is alert and immobilized in a cervical collar. He has hypertension treated with hydrochlorothiazide. His pulse is 90/min and regular, respirations are 18/min, and blood pressure is 140/70 mmHg. Examination shows bruising and midline cervical tenderness. Neurologic examination shows diminished strength and sensation to pain and temperature in the upper extremities, particularly in the hands. Upper extremity deep tendon reflexes are absent. Strength, sensation, and reflexes in the lower extremities are intact. Anal sensation and tone are present. Babinski's sign is absent bilaterally. Which of the following is most likely to confirm the cause of this patient's neurologic examination findings?
Practice by Chapter
Skeletal radiologic landmarks
Practice Questions
Thoracic radiologic landmarks
Practice Questions
Cardiac radiologic landmarks
Practice Questions
Abdominal radiologic landmarks
Practice Questions
Neurological radiologic landmarks
Practice Questions
Pelvic radiologic landmarks
Practice Questions
Spinal radiologic landmarks
Practice Questions
Musculoskeletal radiologic landmarks
Practice Questions
Vascular radiologic landmarks
Practice Questions
Contrast-enhanced landmark identification
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app