
Cardiac radiologic landmarks — MCQs

A 52-year-old man presents to a medical clinic to establish care. He has no known chronic illnesses but has not seen a physician in over 20 years. He generally feels well but occasionally has shortness of breath when he jogs and exercises. He smokes 2-5 cigarettes per day and uses IV heroin “now and then.” Physical exam is unremarkable. ECG shows prominent QRS voltage and left axis deviation. Trans-thoracic echocardiogram shows mild concentric left ventricular hypertrophy but is otherwise normal. Which of the following is the most likely etiology of the echocardiogram findings?
A 42-year-old woman comes to the physician because of 2 episodes of loss of consciousness over the past week. She recovered immediately and was not confused following the episodes. During the past 5 months, she has also had increased shortness of breath and palpitations. She has been unable to carry out her daily activities. She also reports some chest tightness that resolves with rest. She has no history of serious illness and takes no medications. She immigrated with her family from India 10 years ago. Her temperature is 37.3°C (99.1°F), pulse is 115/min and irregular, and blood pressure is 108/70 mm Hg. Examination shows jugular venous distention and pitting edema below the knees. Bilateral crackles are heard at the lung bases. Cardiac examination shows an accentuated and split S2. There is an opening snap followed by a low-pitched diastolic murmur in the fifth left intercostal space at the midclavicular line. An ECG shows atrial fibrillation and right axis deviation. Which of the following is the most likely underlying mechanism of these findings?
A tall, slender 32-year-old man comes to the emergency room because of sudden chest pain, cough, and shortness of breath. On physical examination, he has decreased breath sounds on the right. Chest radiography shows translucency on the right side of his chest. His pCO2 is elevated and pO2 is decreased. What is the most likely cause of his symptoms?
A 64-year-old man presents to the office for an annual physical examination. He has no complaints at this visit. His chart states that he has a history of hypertension, chronic obstructive pulmonary disease (emphysema), Raynaud’s disease, and glaucoma. He is a 30 pack-year smoker. His medications included lisinopril, tiotropium, albuterol, nifedipine, and latanoprost. The blood pressure is 139/96 mm Hg, the pulse is 86/min, the respiration rate is 16/min, and the temperature is 37.2°C (99.1°F). On physical examination, his pupils are equal, round, and reactive to light. The cardiac auscultation reveals an S4 gallop without murmur, and the lungs are clear to auscultation bilaterally. However, the inspection of the chest wall shows an enlarged anterior to posterior diameter. Which of the following is the most appropriate screening test for this patient?
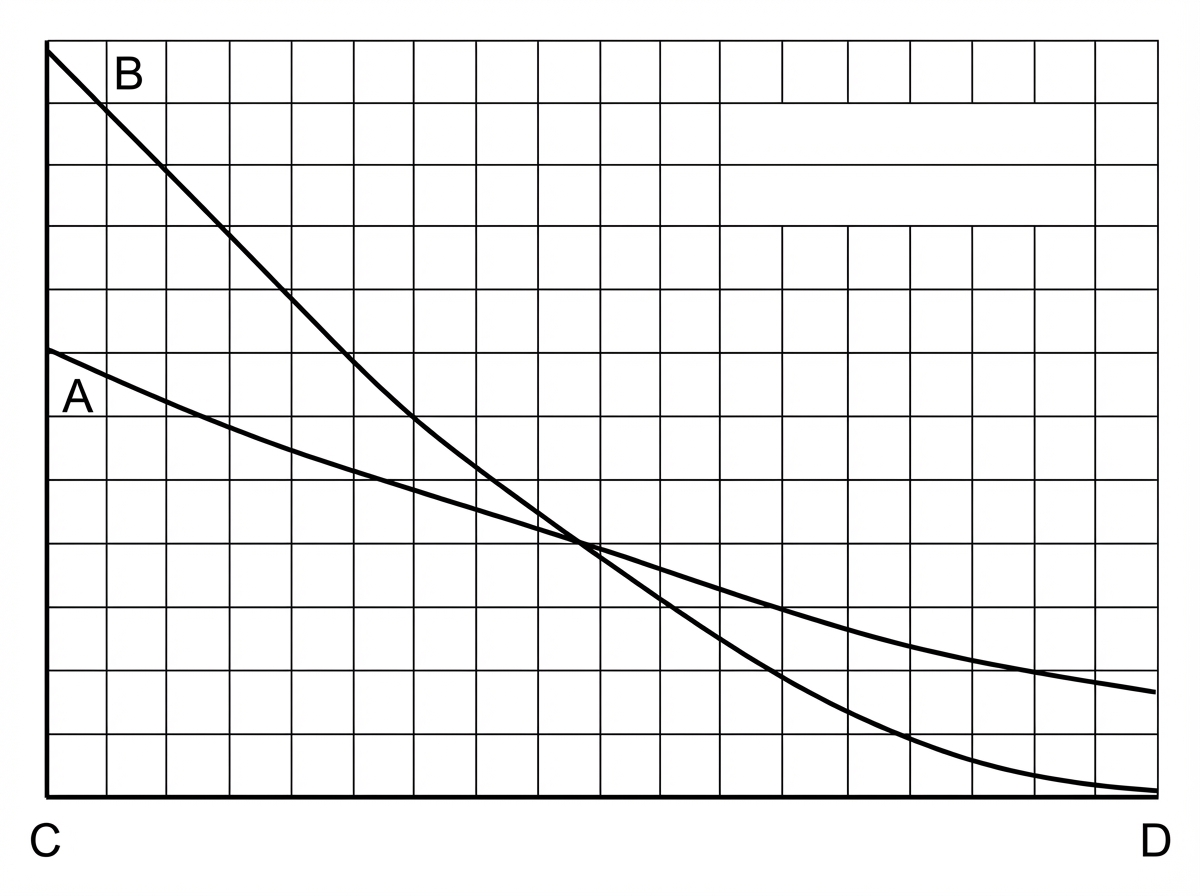
A young researcher is responsible for graphing laboratory data involving pulmonary blood flow and ventilation pattern obtained from a healthy volunteer who was standing in an upright position. After plotting the following graph, the researcher realizes he forgot to label the curves and the x-axis (which represents the position in the lung). Which of the following is the appropriate label for each point on the graph?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
A 2-year-old child is brought to the emergency department with rapid breathing and a severe cyanotic appearance of his lips, fingers, and toes. He is known to have occasional episodes of mild cyanosis, especially when he is extremely agitated. This is the worst episode of this child’s life, according to his parents. He was born with an APGAR score of 8 via a normal vaginal delivery. His development is considered delayed compared to children of his age. History is significant for frequent squatting after strenuous activity. On auscultation, there is evidence of a systolic ejection murmur at the left sternal border. On examination, his oxygen saturation is 71%, blood pressure is 81/64 mm Hg, respirations are 42/min, pulse is 129/min, and temperature is 36.7°C (98.0°F). Which of the following will most likely be seen on chest x-ray (CXR)?
A 55-year-old man visits the clinic with his wife. He has had difficulty swallowing solid foods for the past 2 months. His wife adds that his voice is getting hoarse but they thought it was due to his recent flu. His medical history is significant for type 2 diabetes mellitus for which he is on metformin. He suffered from many childhood diseases due to lack of medical care and poverty. His blood pressure is 125/87 mm Hg, pulse 95/min, respiratory rate 14/min, and temperature 37.1°C (98.7°F). On examination, an opening snap is heard over the cardiac apex. An echocardiogram shows an enlarged cardiac chamber pressing into his esophagus. Changes in which of the following structures is most likely responsible for this patient’s symptoms?
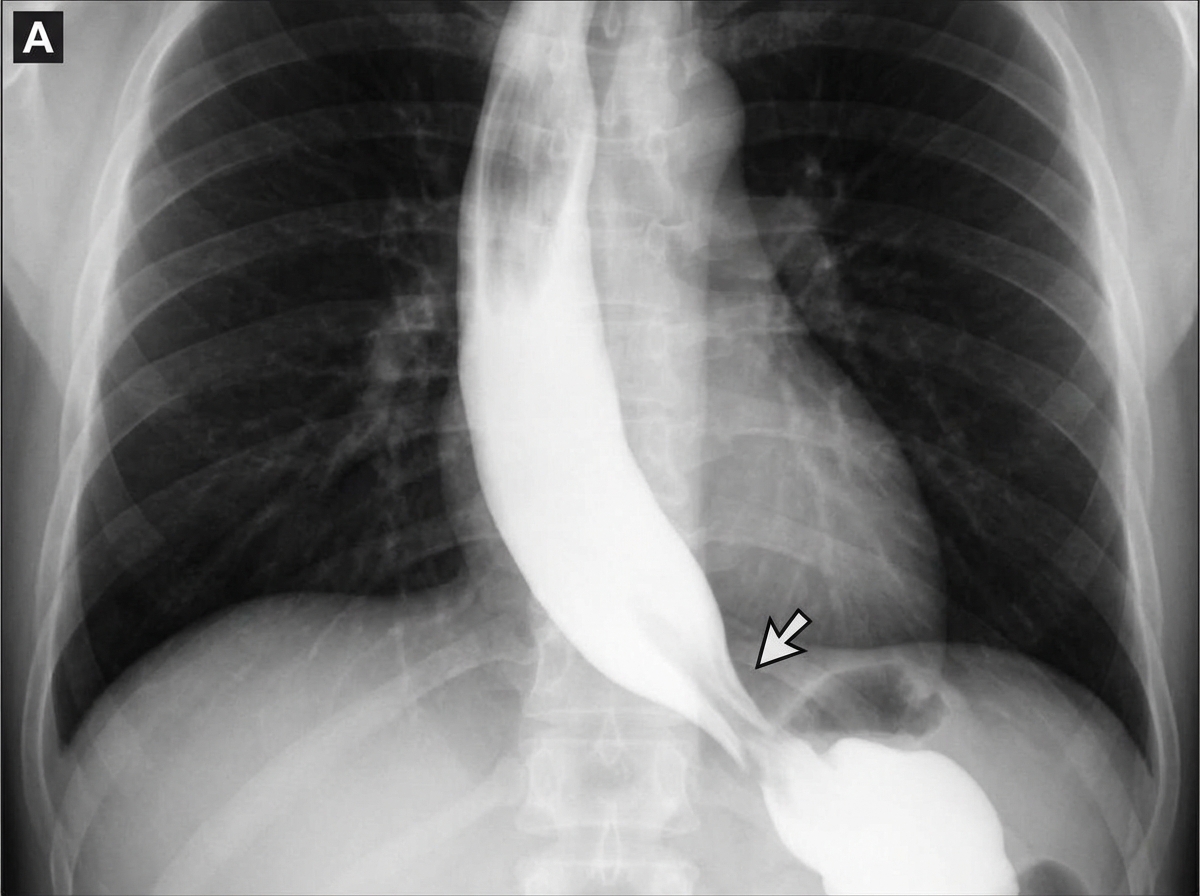
A 45-year-old woman comes to the physician because of progressive difficulty swallowing solids and liquids over the past 4 months. She has lost 4 kg (9 lb) during this period. There is no history of serious illness. She emigrated to the US from Panama 7 years ago. She does not smoke cigarettes or drink alcohol. Cardiopulmonary examination shows a systolic murmur and an S3 gallop. A barium radiograph of the chest is shown. Histopathologic examination of the esophageal wall is most likely to show which of the following?
A 70-year-old woman presents with substernal chest pain. She says that the symptoms began 2 hours ago and have not improved. She describes the pain as severe, episodic, and worse with exertion. She reports that she has had multiple similar episodes that have worsened and increased in frequency over the previous 4 months. Past medical history is significant for diabetes and hypertension, both managed medically. The vital signs include temperature 37.0°C (98.6°F), blood pressure 150/100 mm Hg, pulse 80/min, and respiratory rate 15/min. Her serum total cholesterol is 280 mg/dL and high-density lipoprotein (HDL) is 30 mg/dL. The electrocardiogram (ECG) shows ST-segment depression on multiple chest leads. Coronary angiography reveals 75% narrowing of her left main coronary artery. In which of the following anatomical locations is a mural thrombus most likely to form in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app