
Pharyngeal arches — MCQs

On this page
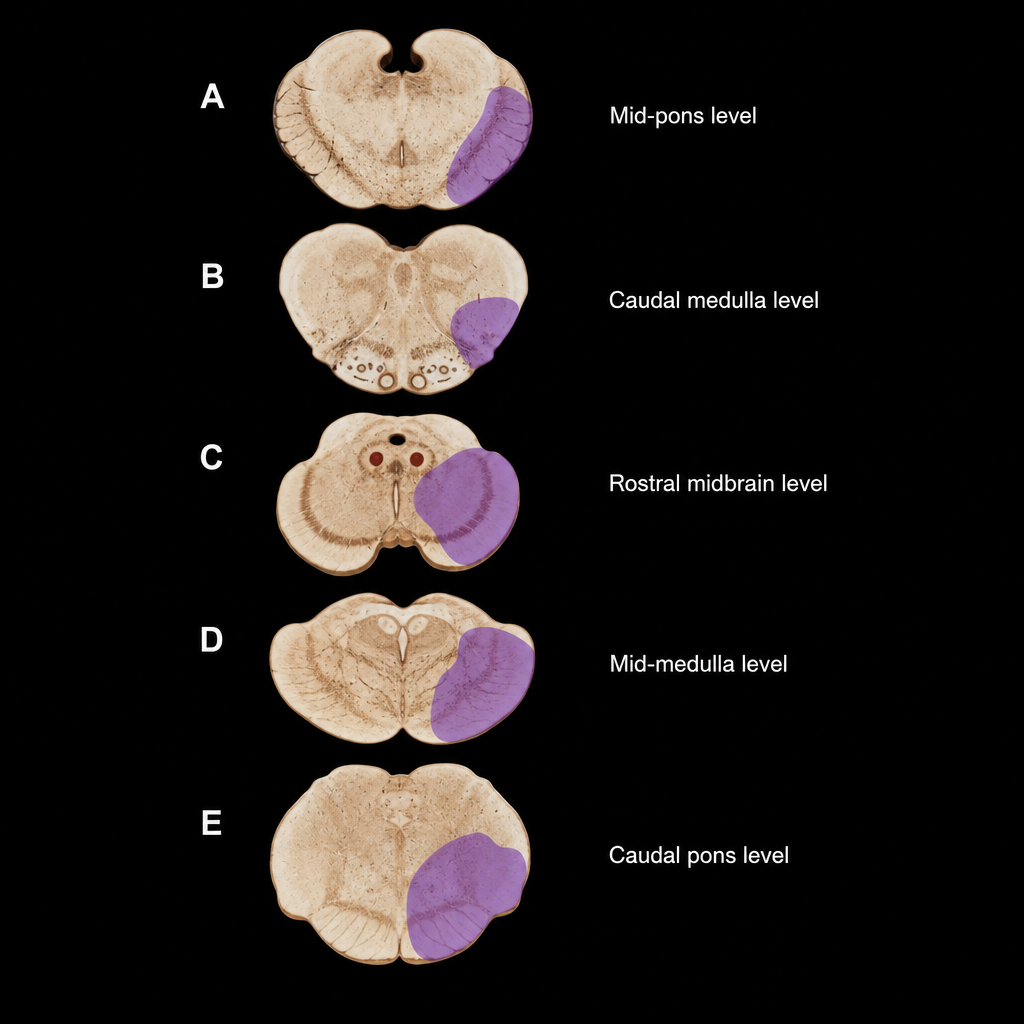
The axial brainstem section shown in the image demonstrates a focal infarct (shaded region) at the level indicated by the label. The patient presents with ipsilateral facial numbness, ipsilateral Horner syndrome, dysphagia, and contralateral loss of pain and temperature sensation in the limbs. At which labelled axial level does this lesion reside, and which artery is most likely occluded?
A 64-year-old woman presents to an endocrinologist after her second time having a kidney stone in the last year. The patient reports no other symptoms except overall fatigue. On evaluation, the patient’s temperature is 98.4°F (36.9°C), blood pressure is 120/76 mmHg, pulse is 72/min, and respirations are 12/min. The patient has no neck masses and no tenderness to palpation in the abdomen. On laboratory workup, the endocrinologist finds that the patient has elevated parathyroid hormone levels and serum calcium. For surgical planning, the patient undergoes a sestamibi scan, which localizes disease to an area near the superior aspect of the thyroid in the right neck. Which of the following is the embryologic origin of this tissue?
A 78-year-old man comes to the physician because of a change in his voice. His wife says his voice has progressively become higher pitched, and he has had a 5.4-kg (11.9-lb) weight loss over the past 4 months. He has smoked half a pack of cigarettes daily for the past 40 years. Direct laryngoscopy shows an irregular, nodular glottic mass. A biopsy specimen of the mass shows poorly differentiated squamous cells with nuclear atypia, hyperkeratosis, and disruption of the basement membrane. Involvement of a muscle derived from which of the following branchial arches is the most likely cause of his symptoms?
A 4-year-old girl is brought by her mother to the pediatrician for neck drainage. The mother reports that the child has always had a small pinpoint opening on the front of her neck, though the opening has never been symptomatic. The child developed a minor cold approximately 10 days ago which resolved after a week. However, over the past 2 days, the mother has noticed clear thick drainage from the opening on the child’s neck. The child is otherwise healthy. She had an uncomplicated birth and is currently in the 45th and 40th percentiles for height and weight, respectively. On examination, there is a small opening along the skin at the anterior border of the right sternocleidomastoid at the junction of the middle and lower thirds of the neck. There is some slight clear thick discharge from the opening. Palpation around the opening elicits a cough from the child. This patient’s condition is caused by tissue that also forms which of the following?
A group of investigators studying embryological defects in mice knock out a gene that is responsible for the development of the ventral wing of the third branchial pouch. A similar developmental anomaly in a human embryo is most likely to result in which of the following findings after birth?
Practice by Chapter
First pharyngeal arch derivatives
Practice Questions
Second pharyngeal arch derivatives
Practice Questions
Third pharyngeal arch derivatives
Practice Questions
Fourth and sixth pharyngeal arch derivatives
Practice Questions
Pharyngeal pouches
Practice Questions
Pharyngeal clefts
Practice Questions
Pharyngeal membrane derivatives
Practice Questions
Neural crest contribution to pharyngeal arches
Practice Questions
Congenital anomalies of pharyngeal arch derivatives
Practice Questions
Clinical correlations of pharyngeal development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app