
GI tract histology — MCQs

A 24-year-old man presents with recurrent abdominal pain, diarrhea with fatty porridge-like stools and occasional blood up to 8 times per day, joint pain, and weight loss. Ileocolonoscopy shows regions of erythema, swelling, and cobblestone-like appearance of the ascending colon and terminal ileum. Targeted biopsies are taken for evaluation. One of the slides, which underwent histological assessment, is shown in the image. Which of the following best describes the histologic finding marked with the blue circle?
A 38-year-old man comes to the clinic complaining of recurrent abdominal pain for the past 2 months. He reports a gnawing, dull pain at the epigastric region that improves with oral ingestion. He has been taking calcium carbonate for the past few weeks; he claims that “it used to help a lot but it’s losing its effects now.” Laboratory testing demonstrated increased gastrin levels after the administration of secretin. A push endoscopy visualized several ulcers at the duodenum and proximal jejunum. What characteristics distinguish the jejunum from the duodenum?
Which of the following cells in the body depends on dynein for its unique functioning?
A 40-year-old female comes in with several months of unintentional weight loss, epigastric pain, and a sensation of abdominal pressure. She has diabetes well-controlled on metformin but no other prior medical history. She has not previously had any surgeries. On physical exam, her doctor notices brown velvety areas of pigmentation on her neck. Her doctor also notices an enlarged, left supraclavicular node. Endoscopic findings show a stomach wall that appears to be grossly thickened. Which of the following findings would most likely be seen on biopsy?
A 34-year-old man presents with a 2-day history of loose stools, anorexia, malaise, and abdominal pain. He describes the pain as moderate, cramping in character, and diffusely localized to the periumbilical region. His past medical history is unremarkable. He works as a wildlife photographer and, 1 week ago, he was in the Yucatan peninsula capturing the flora and fauna for a magazine. The vital signs include blood pressure 120/60 mm Hg, heart rate 90/min, respiratory rate 18/min, and body temperature 38.0°C (100.4°F). Physical examination is unremarkable. Which of the following is a characteristic of the microorganism most likely responsible for this patient’s symptoms?
A 48-year-old female visits your office complaining that she has trouble swallowing solids and liquids, has persistent bad breath, and sometimes wakes up with food on her pillow. Manometry studies show an absence of functional peristalsis and a failure of the lower esophageal sphincter to relax upon swallowing. The patient's disorder is associated with damage to which of the following?
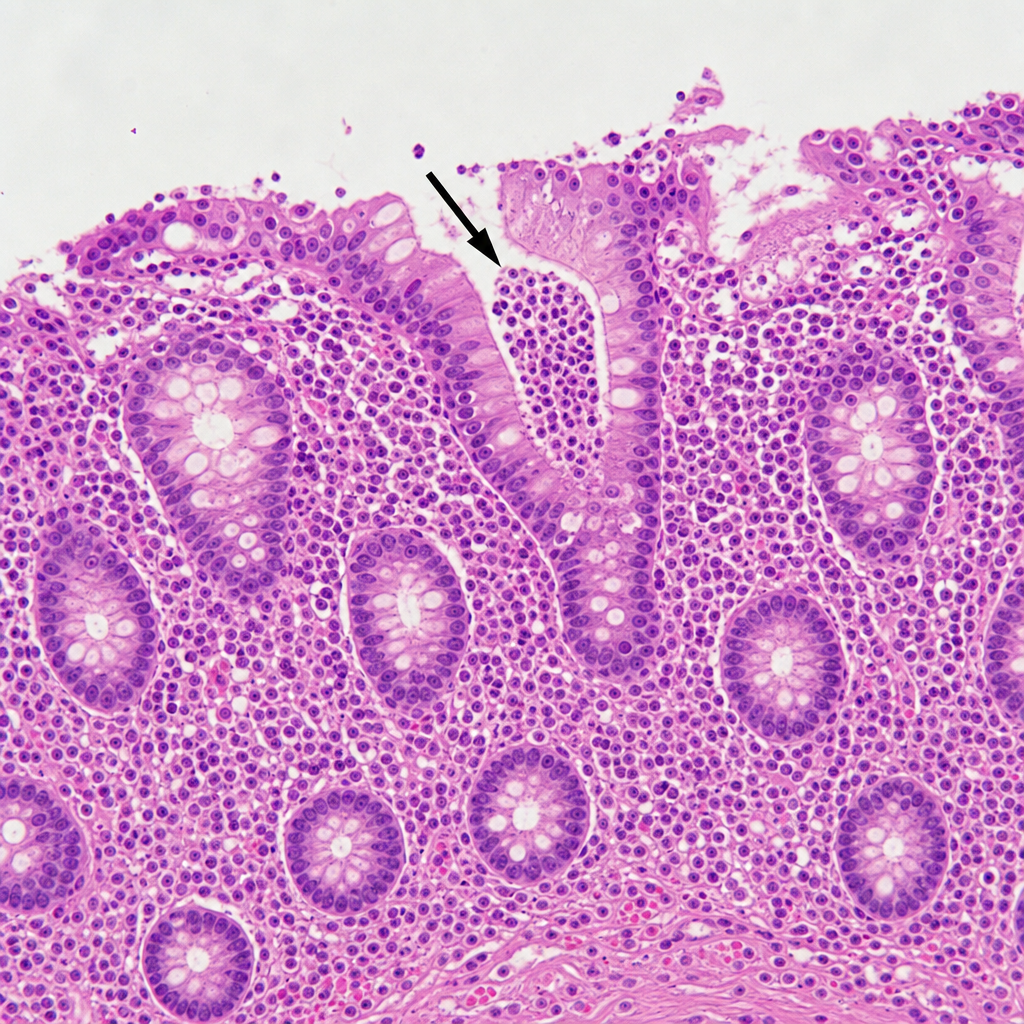
A 52-year-old woman presents with mild epigastric pain and persistent heartburn for the past 2 months. An endoscopy is performed and reveals inflammation of the stomach mucosa without evidence of ulceration. A biopsy is performed and reveals intestinal metaplasia with destruction of a large number of parietal cells. She is diagnosed with chronic atrophic gastritis. Which of the following is characteristic of this patient’s diagnosis?
A 56-year-old man comes to the physician because of intermittent retrosternal chest pain. Physical examination shows no abnormalities. Endoscopy shows salmon pink mucosa extending 5 cm proximal to the gastroesophageal junction. Biopsy specimens from the distal esophagus show nonciliated columnar epithelium with numerous goblet cells. Which of the following is the most likely cause of this patient's condition?
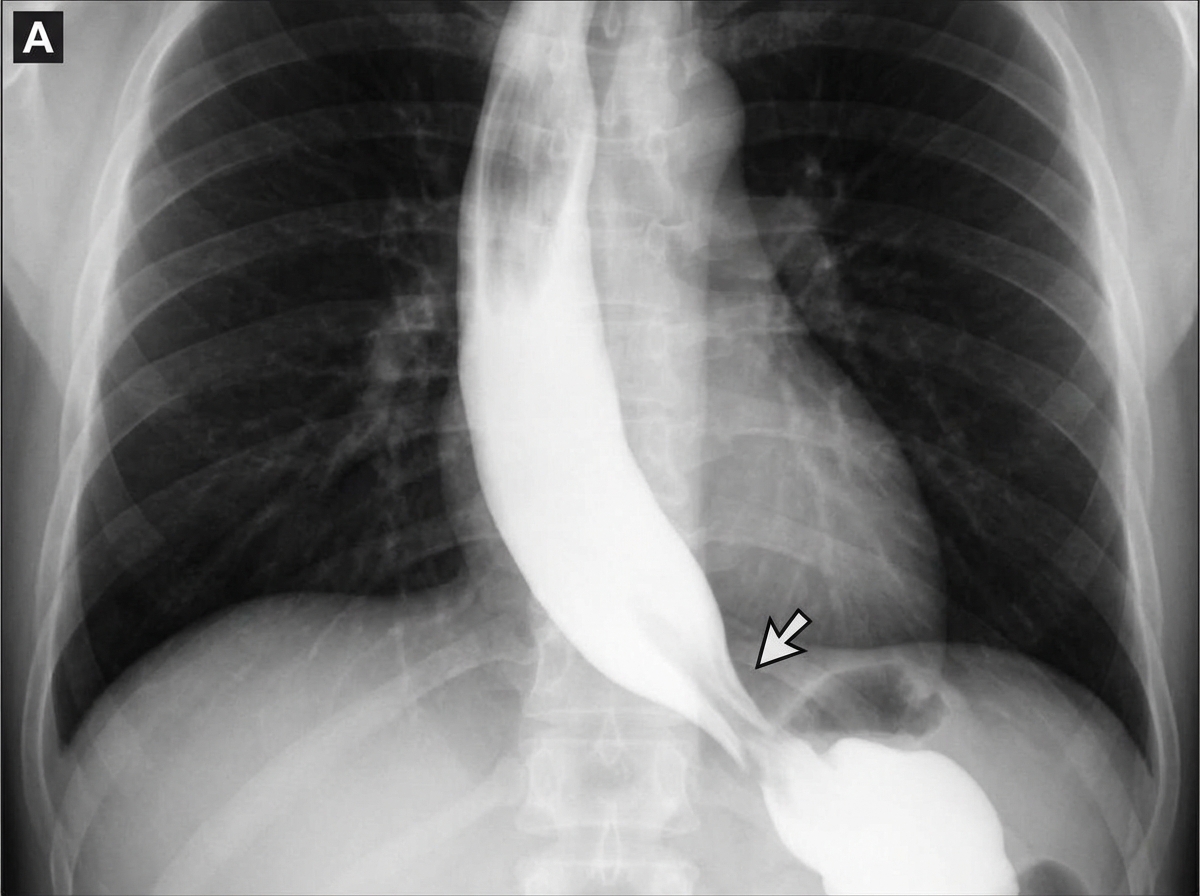
A 45-year-old woman comes to the physician because of progressive difficulty swallowing solids and liquids over the past 4 months. She has lost 4 kg (9 lb) during this period. There is no history of serious illness. She emigrated to the US from Panama 7 years ago. She does not smoke cigarettes or drink alcohol. Cardiopulmonary examination shows a systolic murmur and an S3 gallop. A barium radiograph of the chest is shown. Histopathologic examination of the esophageal wall is most likely to show which of the following?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app