
Neuroanatomy — MCQs

On this page
A 10-year-old boy is brought to the pediatrician by his mother for evaluation. Last night, he was playing with his younger brother and a hot cup of coffee fell on his left shoulder. Though his skin became red and swollen, he acted as if nothing happened and did not complain of pain or discomfort. He has met all expected developmental milestones, and his vaccinations are up-to-date. Physical examination reveals a normal appearing boy with height and weight in the 56th and 64th percentiles for his age, respectively. The skin over his left shoulder is erythematous and swollen. Sensory examination reveals impaired pain and temperature sensation in a cape-like distribution across both shoulders, arms, and neck. The light touch, vibration, and position senses are preserved. The motor examination is within normal limits, and he has no signs of a cerebellar lesion. His gait is normal. Which of the following disorders is most likely associated with this patient’s condition?
A 54-year-old woman comes to the physician because of a 1-day history of fever, chills, and double vision. She also has a 2-week history of headache and foul-smelling nasal discharge. Her temperature is 39.4°C (103°F). Examination shows mild swelling around the left eye. Her left eye does not move past midline on far left gaze but moves normally when looking to the right. Without treatment, which of the following findings is most likely to occur in this patient?
Where does the only cranial nerve without a thalamic relay nucleus enter the skull?
A 52-year-man is brought to the physician because of a 2-week history of memory loss. Three weeks ago, he had a cardiac arrest that required cardiopulmonary resuscitation and intravenous epinephrine. On mental status examination, he cannot recall objects shown to him 20 minutes earlier but vividly recalls memories from before the incident. The remainder of the examination shows no abnormalities. Which of the following structures of the brain is most likely affected?
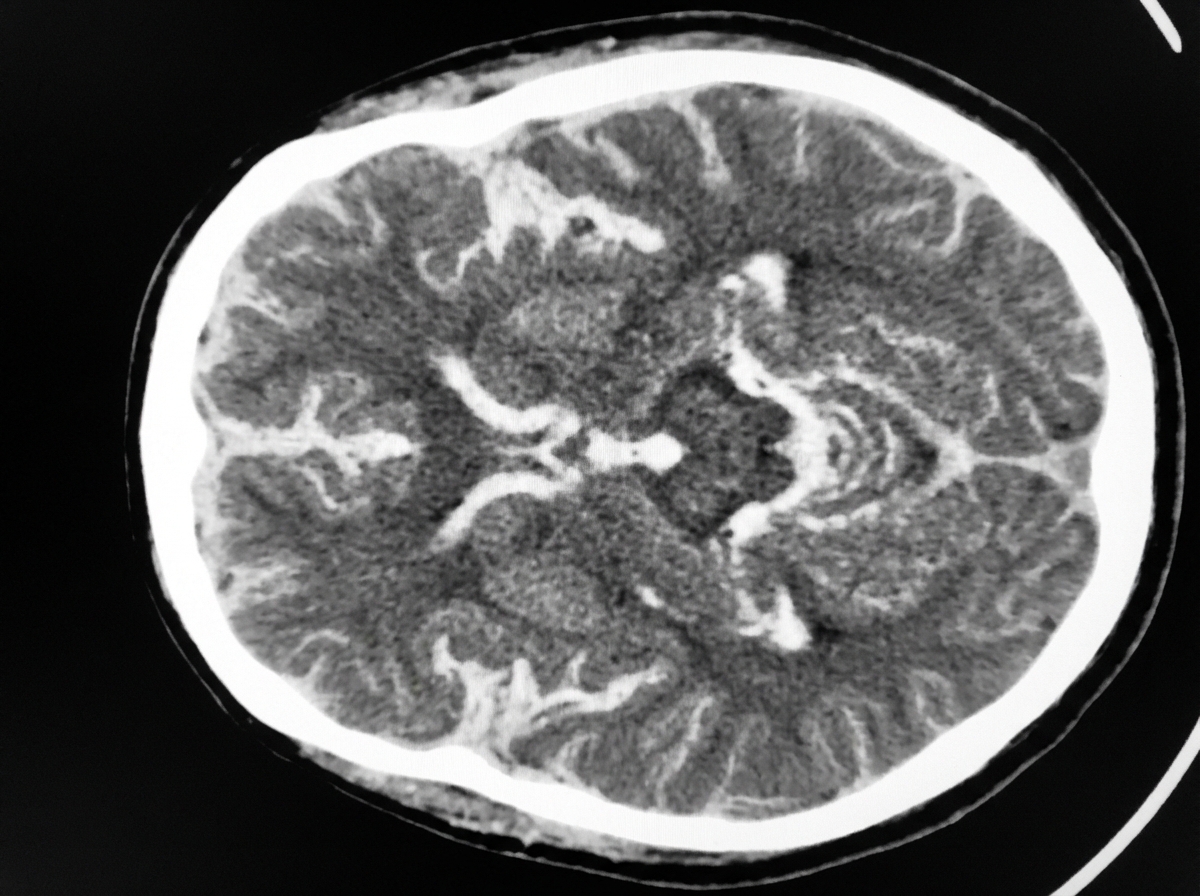
A 54-year-old man is brought to the emergency department 30 minutes after being hit by a car while crossing the street. He had a left-sided tonic-clonic seizure and one episode of vomiting while being transported to the hospital. On arrival, he is not oriented to person, place, or time. Physical examination shows nuchal rigidity and bilateral extensor plantar responses. A CT scan of the head is shown. This patient's symptoms are most likely the result of a hemorrhage in which of the following structures?
A 54-year-old man is referred to a tertiary care hospital with a history of 5 months of progressive difficulty in walking and left leg numbness. He first noticed mild gait unsteadiness and later developed gradual right leg weakness. His left leg developed progressive numbness and tingling. His blood pressure is 138/88 mm Hg, the heart rate is 72/min, and the temperature is 36.7°C (98.2°F). On physical examination, he is alert and oriented to person, place, and time. Cranial nerves are intact. Muscle strength is 5/5 in both upper extremities and left lower extremity, but 3/5 in the right leg with increased tone. The plantar reflex is extensor on the right. Pinprick sensation is decreased on the left side below the umbilicus. Vibration and joint position senses are decreased in the right foot and leg. All sensations are normal in the upper extremities. Finger-to-nose and heel-to-shin testing are normal. This patient’s lesion is most likely located in which of the following parts of the nervous system?
A 67-year-old female patient is brought to the emergency department after her daughter noticed she has been having meaningless speech. When assessing the patient, she calls the chair a table, and at times would make up new words. She does not appear to be aware of her deficit, and is carrying on an empty conversation. Her speech is fluent, but with paraphasic errors. Her repetition is impaired. On physical examination, a right upper quadrant field-cut is appreciated, with impairment in comprehension and repetition. Which of the following structures is most likely involved in this patient’s presentation?
A 67-year-old man is brought to the physician by his daughter because he frequently misplaces his personal belongings and becomes easily confused. His daughter mentions that his symptoms have progressively worsened for the past one year. On mental status examination, he is oriented to person, place, and time. He vividly recalls memories from his childhood but can only recall one of three objects presented to him after 5 minutes. His affect is normal. This patients' symptoms are most likely caused by damage to which of the following?
A 72-year-old man presents to his primary care physician due to worsening headache and double vision. His headache began several months ago, and he describes them as sharp and localized to the left side of the head. His double vision began one week prior to presentation. Medical history is significant for hypertension and type II diabetes mellitus, which is treated with lisinopril and metformin. He smokes a pack of cigarettes a day for the last 40 years. His temperature is 98.3°F (37°C), blood pressure is 148/84 mmHg, pulse is 60/min, and respirations are 14/min. On physical exam, a mild head turning towards the left is appreciated. Pupils are equal, round, and reactive to light, with a more pronounced esotropia on left-lateral gaze. The rest of the neurologic exam is otherwise normal. Magnetic resonance imaging (MRI) of the head and MR angiography shows a left-sided intracavernous carotid aneurysm. Which of the following nerves is most likely compressed by the aneurysm in this patient?
A 35-year-old man who suffered a motor vehicle accident 3 months ago presents to the office for a neurological evaluation. He has no significant past medical history and takes no current medications. He has a family history of coronary artery disease in his father and Alzheimer’s disease in his mother. On physical examination, his blood pressure is 110/60 mm Hg, the pulse is 85/min, the temperature is 37.0°C (98.6°F), and the respiratory rate is 20/min. Neurological examination is suggestive of a lesion in the anterior spinal artery that affects the anterior two-thirds of the spinal cord, which is later confirmed with angiography. Which of the following exam findings would have suggested this diagnosis?
Practice by Chapter
Cerebral cortex and lobes
Practice Questions
Basal ganglia
Practice Questions
Thalamus and hypothalamus
Practice Questions
Limbic system
Practice Questions
Cerebellum
Practice Questions
Spinal cord organization
Practice Questions
CSF production and circulation
Practice Questions
Meninges and blood-brain barrier
Practice Questions
Sensory pathways
Practice Questions
Motor pathways
Practice Questions
Functional neuroanatomy of vision
Practice Questions
Functional neuroanatomy of hearing and balance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app