
Neuroanatomy — MCQs

On this page
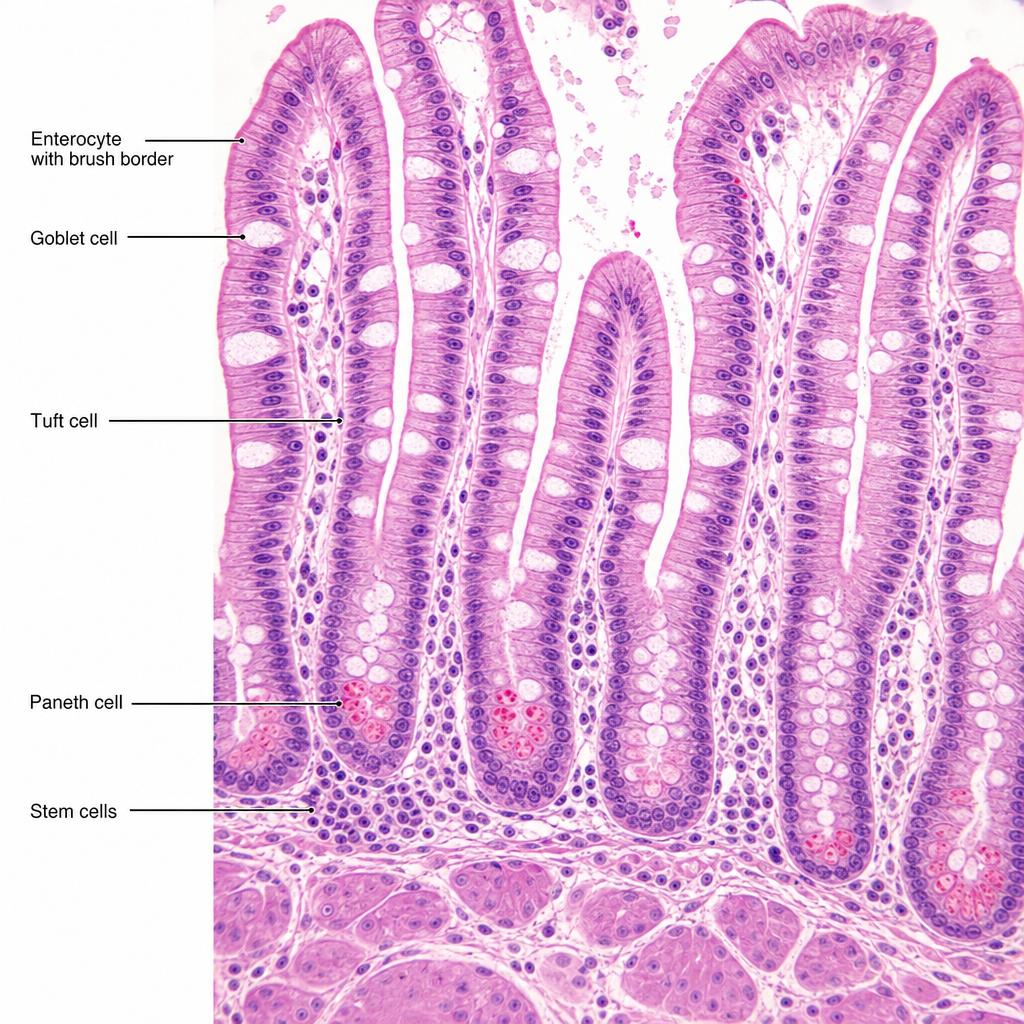
A histology slide from a surgical biopsy of the small intestine reveals tall columnar cells with a prominent brush border, interspersed with flask-shaped cells containing apical mucin granules, and occasional triangular cells wedged at the base of the crypts with eosinophilic granules. A separate population of undifferentiated cells is clustered at the base of the crypts. Based on this architecture, which cell type is responsible for the eosinophilic granules and what is its primary functional role?
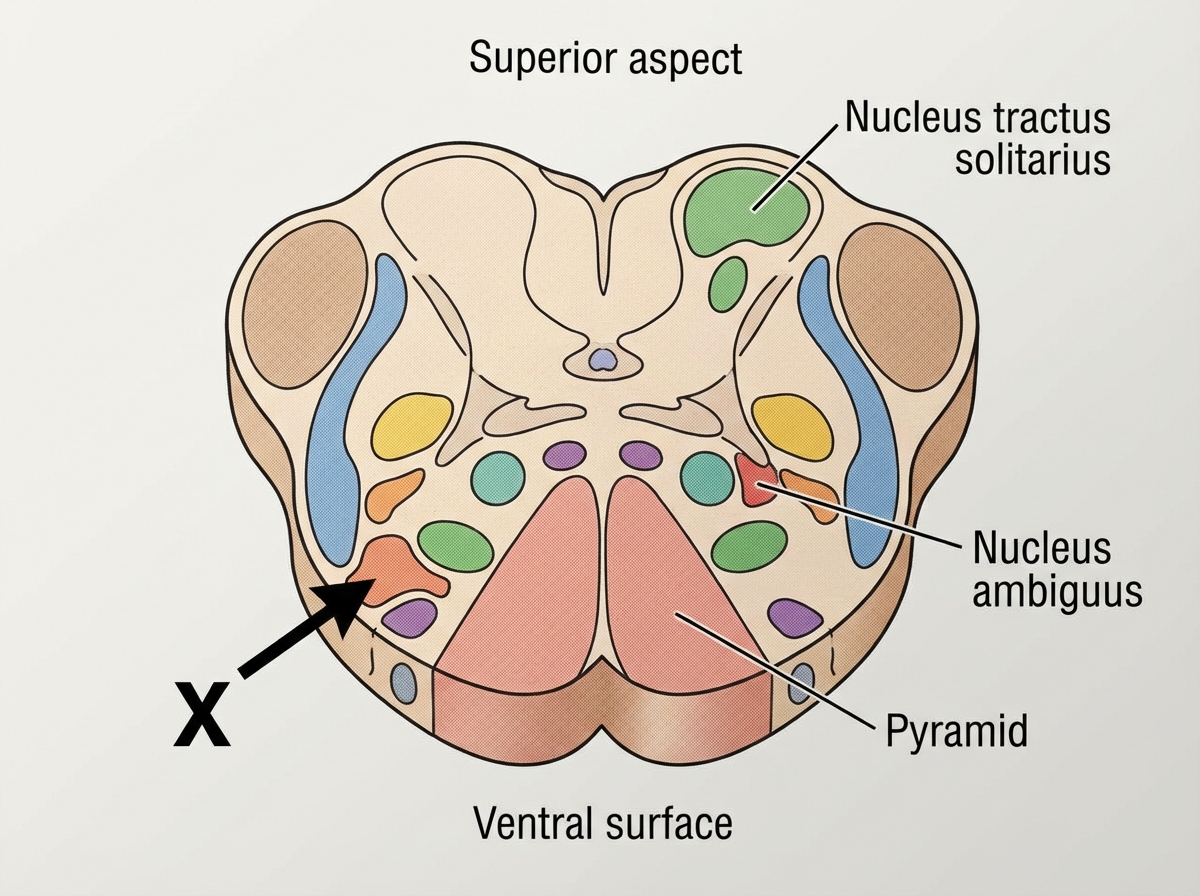
Name the center shown as $X$ in the cut section of medulla which is responsible for control of respiration.
The marked area in the image given below is associated with which part of brain cortex?

Identify the structure shown below. (Recent NEET Pattern 2019)
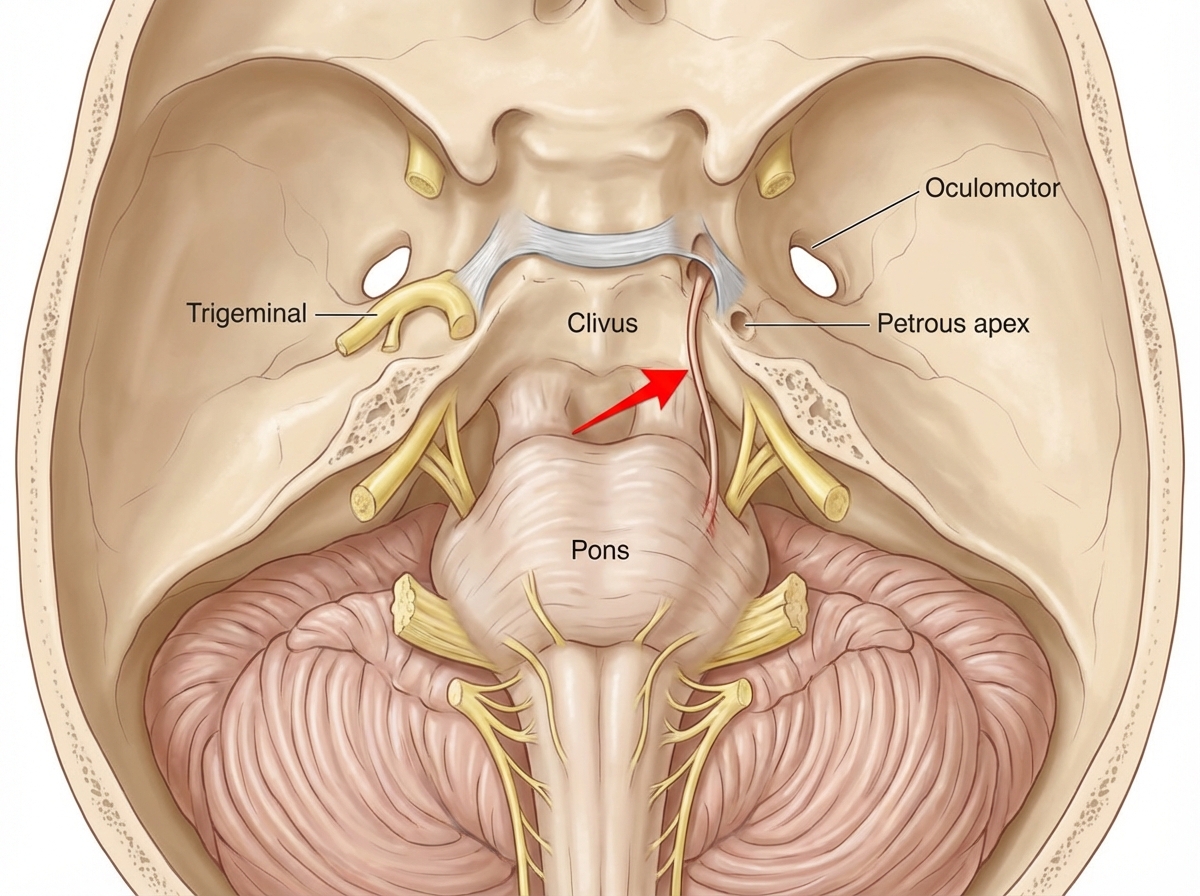
Identify the nerve marked with an arrow in the given section of cranial cavity.
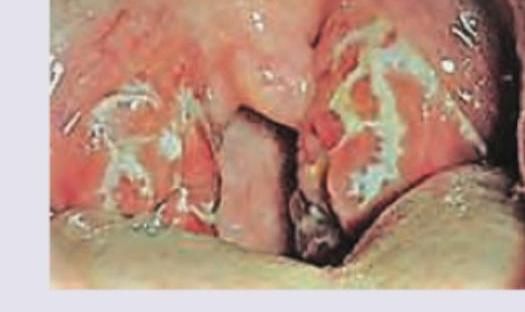
A child is brought with fever and ear pain. On examination following findings are noted. The cranial nerve involved for ear pain is:
A 4-day-old neonate under phototherapy in NICU. The child has shrill cry. All are true about the acute presentation of the disease except:

At what age does maximum brain growth occur?
Arrange in sequence the structures involved in the direct pathway (1=Striatum, 2=GPi, 3=Thalamus, 4=Cortex output, 5=Cortex input):-
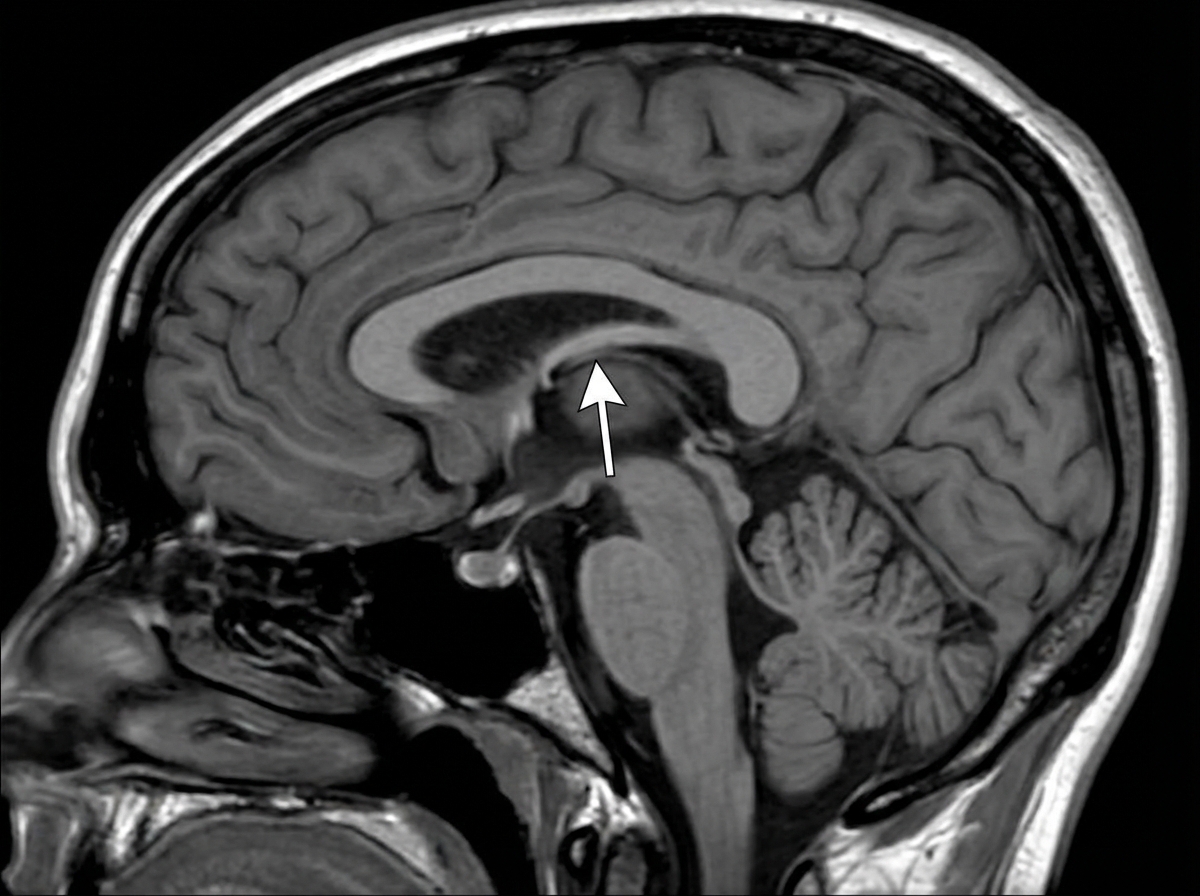
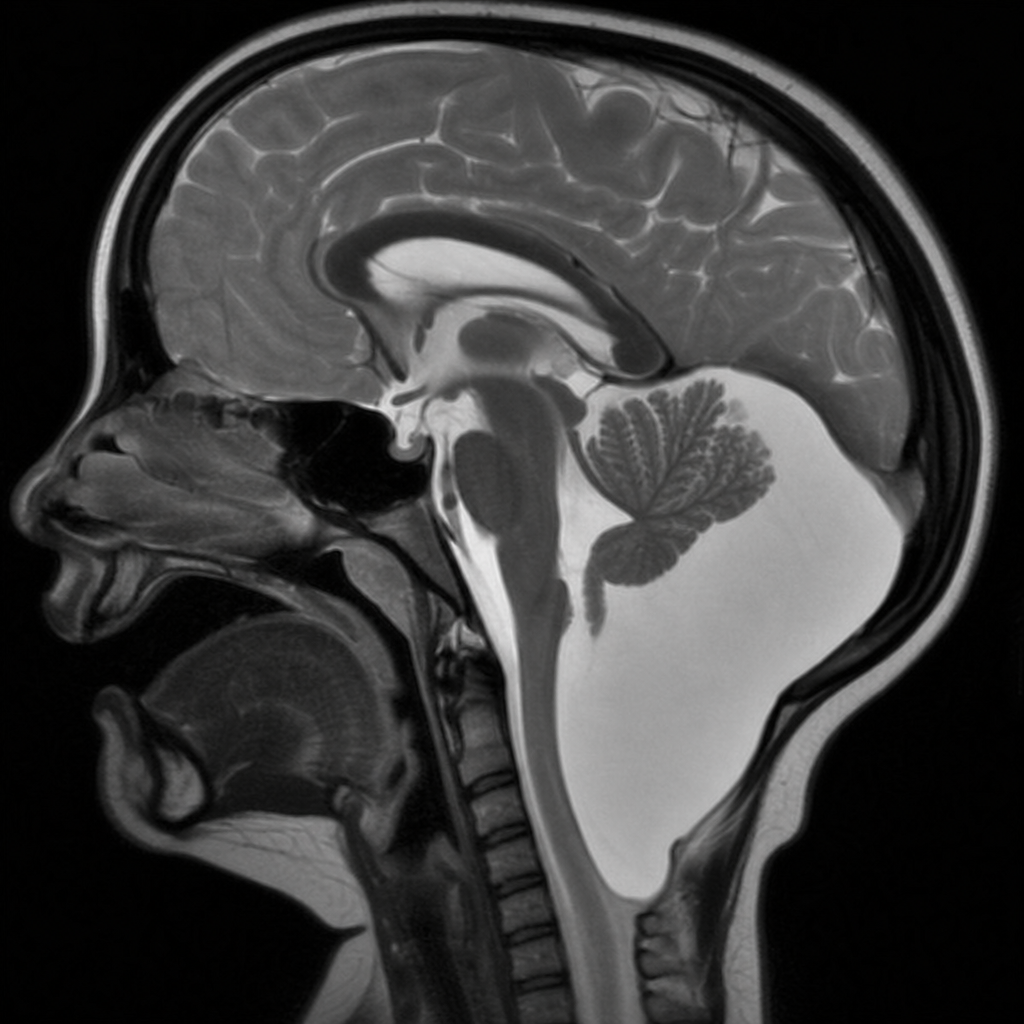
A 2-year-old boy is brought to the physician because of progressive headaches, dizziness, and recurrent episodes of vomiting for 3 weeks. He has a history of surgical removal of a sac-like protuberance on his lower back soon after birth. Neurologic examination shows ataxia. Fundoscopy shows bilateral optic disk swelling. An MRI of the brain is shown. Which of the following is the most likely diagnosis?
Practice by Chapter
Cerebral cortex and lobes
Practice Questions
Basal ganglia
Practice Questions
Thalamus and hypothalamus
Practice Questions
Limbic system
Practice Questions
Cerebellum
Practice Questions
Spinal cord organization
Practice Questions
CSF production and circulation
Practice Questions
Meninges and blood-brain barrier
Practice Questions
Sensory pathways
Practice Questions
Motor pathways
Practice Questions
Functional neuroanatomy of vision
Practice Questions
Functional neuroanatomy of hearing and balance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app