
Lymphedema pathophysiology — MCQs

A 52-year-old man presents to the emergency department because of pain and swelling in his left leg over the past few hours. He traveled from Sydney to Los Angeles 2 days ago. He has had type 2 diabetes mellitus for 10 years and takes metformin for it. He has smoked a pack of cigarettes daily for 25 years. His temperature is 36.9°C (98.4°F), the blood pressure is 140/90 mm Hg, and the pulse is 90/min. On examination, the left calf is 5 cm greater in circumference than the right. The left leg appears more erythematous than the right with dilated superficial veins. Venous duplex ultrasound shows non-compressibility. Which of the following best represents the mechanism of this patient’s illness?
A 76-year-old woman is brought to the physician because of lesions on her left arm. She first noticed them 3 months ago and they have grown larger since that time. She has not had any pain or pruritus in the area. She has a history of invasive ductal carcinoma of the left breast, which was treated with mastectomy and radiation therapy 27 years ago. Since that time, she has had lymphedema of the left arm. Physical examination shows extensive edema of the left arm. There are four coalescing, firm, purple-blue nodules on the left lateral axillary region and swelling of the surrounding skin. Which of the following is the most likely diagnosis?
A 93-year-old woman is brought to the physician because of a purple area on her right arm that has been growing for one month. She has not had any pain or itching of the area. She has hyperlipidemia, a history of basal cell carcinoma treated with Mohs surgery 2 years ago, and a history of invasive ductal carcinoma of the right breast treated with radical mastectomy 57 years ago. She has had chronic lymphedema of the right upper extremity since the mastectomy. Her only medication is simvastatin. She lives in an assisted living facility. She is content with her living arrangement but feels guilty that she is dependent on others. Vital signs are within normal limits. Physical examination shows extensive edema of the right arm. Skin exam of the proximal upper right extremity shows three coalescing, 0.5–1.0 cm heterogeneous, purple-colored plaques with associated ulceration. Which of the following is the most likely diagnosis?
Two weeks after undergoing low anterior resection for rectal cancer, a 52-year-old man comes to the physician because of swelling in both feet. He has not had any fever, chills, or shortness of breath. His temperature is 36°C (96.8°F) and pulse is 88/min. Physical examination shows a normal thyroid and no jugular venous distention. Examination of the lower extremities shows bilateral non-pitting edema that extends from the feet to the lower thigh, with deep flexion creases. His skin is warm and dry, and there is no erythema or rash. Microscopic examination of the interstitial space in this patient's lower extremities would be most likely to show the presence of which of the following?
A 54-year-old man comes to the emergency department because of a 3-week history of intermittent swelling of his left arm and feeling of fullness in his head that is exacerbated by lying down and bending over to tie his shoes. Physical examination shows left-sided facial edema and distention of superficial veins in the neck and left chest wall. Which of the following is the most likely cause of this patient's symptoms?
A 65-year-old man presents with painless swelling of the neck over the past week. He also has noted severe night sweats, which require a change of clothes and bed linens the next day. His medical history is significant for long-standing hypertension. He received a kidney transplant 6 years ago. His current medications include amlodipine, metoprolol, furosemide, aspirin, tacrolimus, and mycophenolate. His family history is significant for his sister, who died last year from lymphoma. A review of systems is positive for a 6-kg (13.2-lb) unintentional weight loss over the past 2 months. His vital signs include: temperature 37.8°C (100.0°F) and blood pressure 120/75 mm Hg. On physical examination, there are multiple painless lymph nodes, averaging 2 cm in diameter, palpable in the anterior and posterior triangles of the neck bilaterally. Axillary and inguinal lymphadenopathy is palpated on the right side. Abdominal examination is significant for a spleen of 16 cm below the costal margin on percussion. Laboratory studies are significant for the following: Hemoglobin 9 g/dL Mean corpuscular volume 88 μm3 Leukocyte count 12,000/mm3 Platelet count 130,000/mm3 Creatinine 1.1 mg/dL Lactate dehydrogenase (LDH) 1,000 U/L A peripheral blood smear is unremarkable. Which of the following is the most likely diagnosis in this patient?
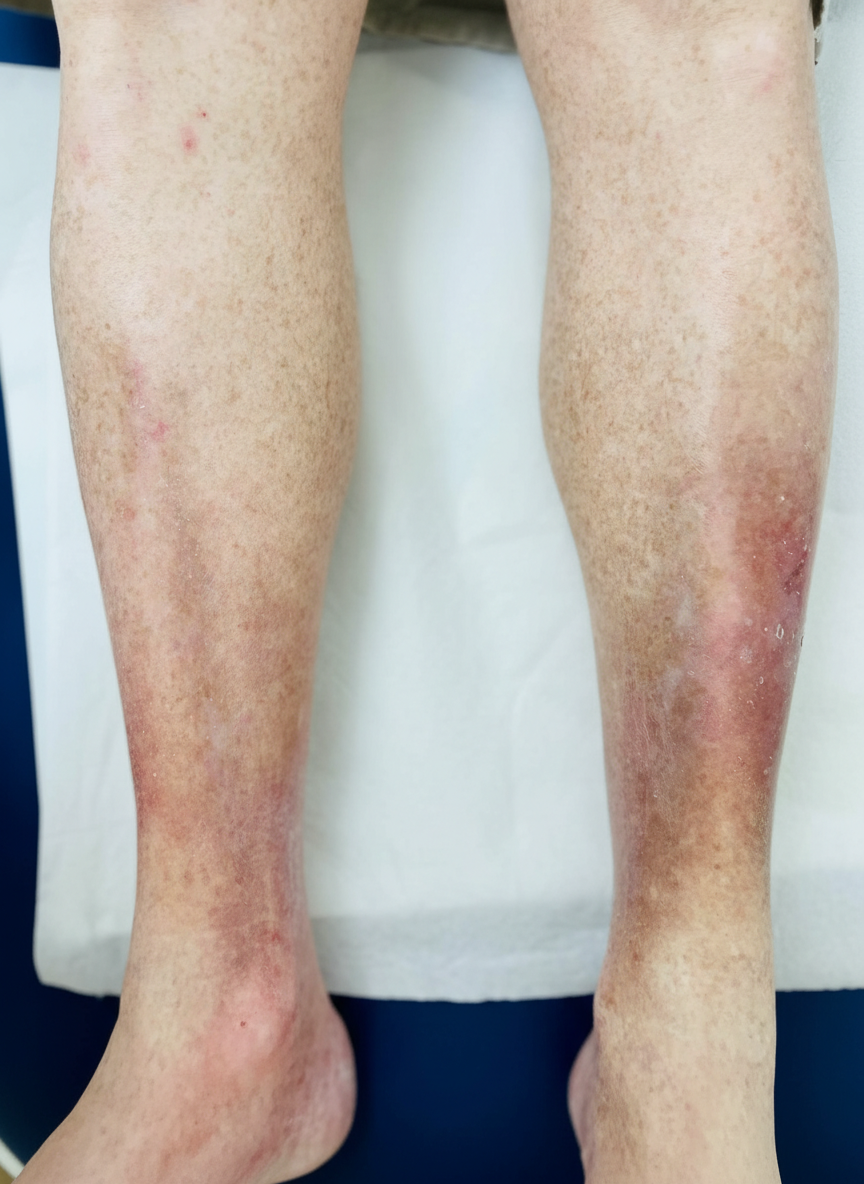
A 67-year-old woman comes to the physician with a 6-month history of pain and swelling of both legs. The symptoms are worst at the end of the day and are associated with itching of the overlying skin. Physical examination shows bilateral pitting ankle edema. An image of one of the ankles is shown. This patient is at greatest risk for which of the following complications?
A 23-year-old woman presents to her primary care physician with 3 days of fatigue and back pain after she started a drug for malaria prophylaxis. She says that her urine has also been darker over the same time period. Her past medical history is significant for allergies as well as a broken elbow that was treated in a cast 10 years ago. She does not take any medications, does not smoke, and drinks socially. Peripheral blood smear reveals both red blood cells with dark intracellular inclusions as well as abnormally shaped red blood cells. The immune cells responsible for the shape of these red blood cells are located in which of the following places?
A 44-year-old woman undergoes radical hysterectomy for stage IB2 cervical cancer. During surgery, the gynecologic oncologist notes aberrant lymphatic drainage patterns possibly related to the patient's history of pelvic inflammatory disease and previous cesarean section. Frozen section of a lymph node from the obturator fossa shows metastatic disease. Synthesizing knowledge of primary and collateral cervical lymphatic drainage, which nodal group represents the most critical next level of drainage that would impact surgical decision-making?
A 67-year-old man with squamous cell carcinoma of the anal canal presents for staging. Physical examination reveals a 3 cm tumor at the dentate line extending both above and below it. Inguinal lymphadenopathy is palpable bilaterally. CT shows both inguinal and pelvic lymph node enlargement. Evaluating the lymphatic drainage of the anal canal, which treatment approach best addresses the dual drainage patterns of this tumor location?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app