
Head and neck lymphatics — MCQs

A 68-year-old man comes to the physician because of a 6-month history of difficulty swallowing pieces of meat and choking frequently during meal times. He also sometimes regurgitates foul-smelling, undigested food particles. Examination shows a 3 x 3 cm soft cystic, immobile mass in the upper third of the left side of his neck anterior to the left sternocleidomastoid muscle that becomes prominent when he coughs. A barium swallow shows an accumulation of contrast on the lateral aspect of the neck at the C5 level. Which of the following is the most likely underlying cause for this patient's condition?
A 32-year-old man comes to the physician because of a 3-week history of cough, weight loss, and night sweats. He migrated from Sri Lanka 6 months ago. He appears emaciated. His temperature is 38.1°C (100.5°F). Physical examination shows enlargement of the right supraclavicular lymph node. Chest and abdominal examination show no abnormalities. An interferon-gamma assay is positive. A biopsy specimen of the cervical lymph node is most likely to show the causal organism in which of the following locations?
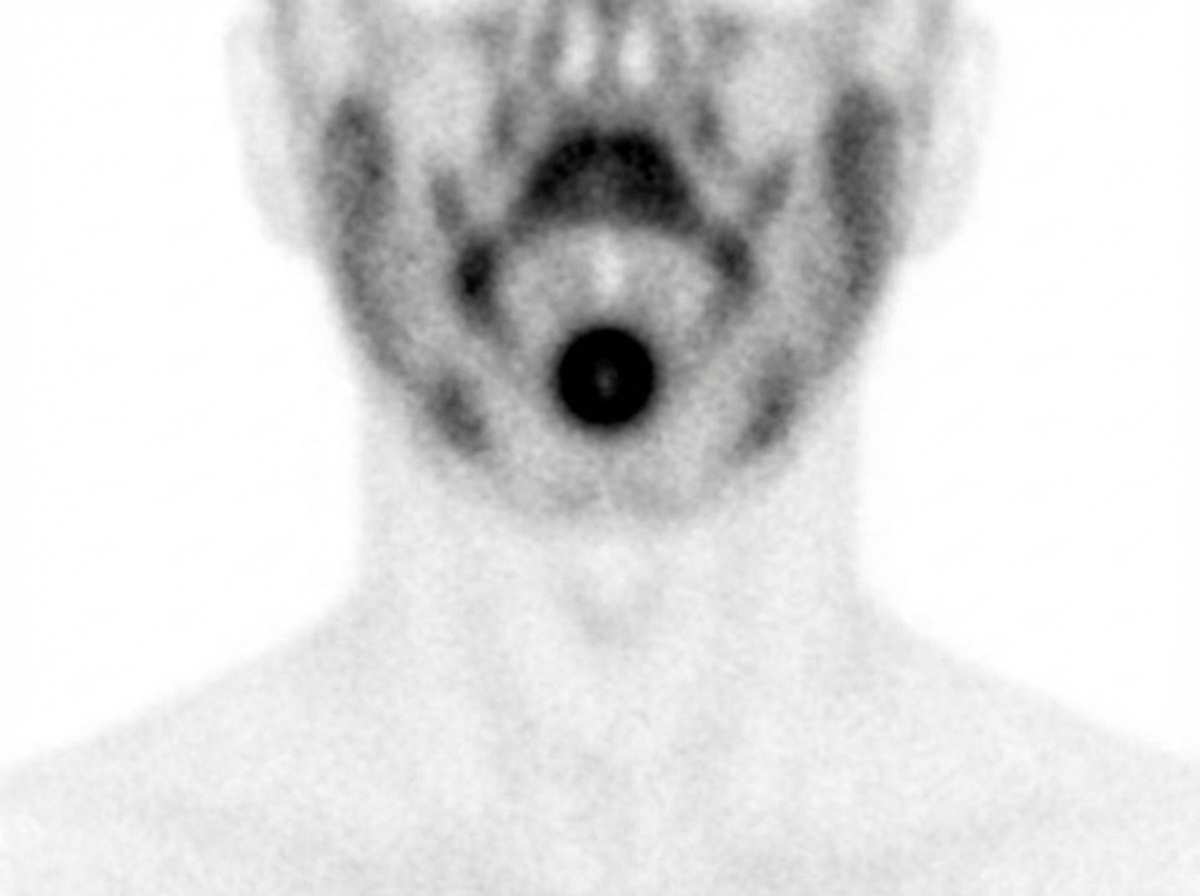
A 16-year-old boy comes to the physician because of a 1-week history of difficulty swallowing, a foreign body sensation at the back of his throat, and trouble breathing at night. He has just recovered from an upper respiratory tract infection that began 5 days ago. On questioning, he reports that he has had similar symptoms in the past each time he has had an upper respiratory tract infection. Physical examination shows a 3 x 2-cm, nontender, rubbery midline mass at the base of the tongue. His skin is dry and cool. An image of his technetium-99m pertechnetate scan is shown. Which of the following is the most likely underlying cause of this patient’s condition?
A 76-year-old woman comes to the physician for evaluation of a 3-month history of vulvar itching and pain. She was diagnosed with lichen sclerosus 4 years ago. She has smoked 1 pack of cigarettes daily for 35 years. Physical examination shows a 2.5-cm nodular, ulcerative lesion on the vaginal introitus and left labia minora with surrounding erythema. Punch biopsy shows squamous cell carcinoma. A CT scan of the chest, abdomen, and pelvis shows enlarged lymph nodes concerning for metastatic disease. Which of the following lymph node regions is the most likely primary site of metastasis?
A 47-year-old man presents to you with gradual loss of voice and difficulty swallowing for the past couple of months. The difficulty of swallowing is for both solid and liquid foods. His past medical history is insignificant except for occasional mild headaches. Physical exam also reveals loss of taste sensation on the posterior third of his tongue and palate, weakness in shrugging his shoulders, an absent gag reflex, and deviation of the uvula away from the midline. MRI scanning was suggested which revealed a meningioma that was compressing some cranial nerves leaving the skull. Which of the following openings in the skull transmit the affected cranial nerves?
A 34-year-old man comes to the physician because of progressive swelling of the left lower leg for 4 months. One year ago, he had an episode of intermittent fever and tender lymphadenopathy that occurred shortly after he returned from a trip to India and resolved spontaneously. Physical examination shows 4+ nonpitting edema of the left lower leg. His leukocyte count is 8,000/mm3 with 25% eosinophils. A blood smear obtained at night confirms the diagnosis. Treatment with diethylcarbamazine is initiated. Which of the following is the most likely route of transmission of the causal pathogen?
A 44-year-old woman undergoes radical hysterectomy for stage IB2 cervical cancer. During surgery, the gynecologic oncologist notes aberrant lymphatic drainage patterns possibly related to the patient's history of pelvic inflammatory disease and previous cesarean section. Frozen section of a lymph node from the obturator fossa shows metastatic disease. Synthesizing knowledge of primary and collateral cervical lymphatic drainage, which nodal group represents the most critical next level of drainage that would impact surgical decision-making?
A 67-year-old man with squamous cell carcinoma of the anal canal presents for staging. Physical examination reveals a 3 cm tumor at the dentate line extending both above and below it. Inguinal lymphadenopathy is palpable bilaterally. CT shows both inguinal and pelvic lymph node enlargement. Evaluating the lymphatic drainage of the anal canal, which treatment approach best addresses the dual drainage patterns of this tumor location?
A 38-year-old woman presents with a firm, fixed thyroid mass. Fine needle aspiration suggests papillary thyroid carcinoma. Ultrasound reveals suspicious lymph nodes in multiple cervical levels. She has a history of total laryngectomy for laryngeal cancer 5 years ago, which altered her cervical lymphatic drainage. Synthesizing knowledge of both normal and altered lymphatic pathways, which nodal station would be LEAST likely to be involved by direct thyroid lymphatic spread in this patient?
A 48-year-old woman presents with a pigmented lesion on the plantar surface of her right heel. Biopsy reveals melanoma with a Breslow depth of 2.5 mm. Sentinel lymph node biopsy is planned. However, during lymphoscintigraphy, tracer uptake is seen in two separate nodal basins. Which anatomic explanation best accounts for this dual drainage pattern from the heel?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app