
Heart development — MCQs

On this page
A 27-year-old G2P1 female gives birth to a baby girl at 33 weeks gestation. The child is somnolent with notable difficulty breathing. Pulse pressure is widened. She is profusely cyanotic. Auscultation is notable for a loud single S2. An echocardiogram demonstrates an enlarged heart and further studies show blood from the left ventricle entering the pulmonary circulation as well as the systemic circulation. Which of the following processes was most likely abnormal in this patient?
Shortly after delivery, a female newborn develops bluish discoloration of the lips, fingers, and toes. She was born at term to a 38-year-old primigravid woman. Pregnancy was complicated by maternal diabetes mellitus. Pulse oximetry on room air shows an oxygen saturation of 81%. Echocardiography shows immediate bifurcation of the vessel arising from the left ventricle; the vessel emerging from the right ventricle gives out coronary, head, and neck vessels. An abnormality in which of the following developmental processes most likely accounts for this patient's condition?
A 2-year-old girl is brought to the emergency department by her mother after an episode of turning blue on the playground. The mother states that the girl starting crying, and her fingers and hands turned blue. On examination, the patient is playful and in no apparent distress. She is afebrile and the vital signs are stable. The lungs are clear to auscultation bilaterally with no evidence of respiratory distress. There is a fixed, split S2 heart sound on cardiac exam without the presence of a S3 or S4. The peripheral pulses are equal bilaterally. What is the underlying cause of this patient’s presentation?
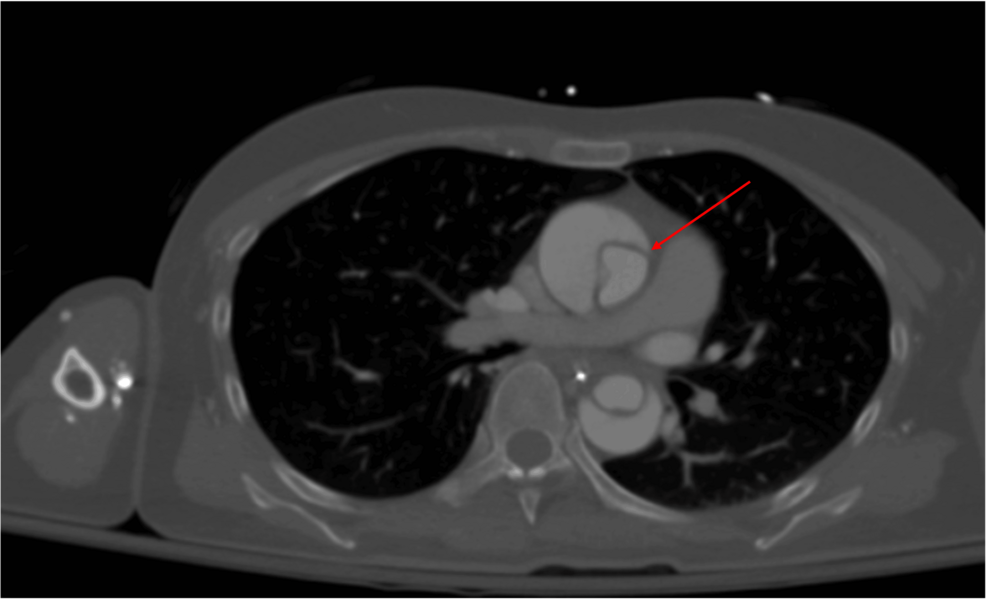
A 56-year-old man is brought to the emergency department 25 minutes after the sudden onset of severe pain in the middle of his chest. He describes the pain as tearing in quality; it radiates to his jaw. He has hypertension. He has smoked one pack of cigarettes daily for the 25 years. Current medications include enalapril. His blood pressure is 154/95 mm Hg in his right arm and 181/105 mm Hg in his left arm. A CT scan of the chest is shown. The structure indicated by the arrow is a derivative of which of the following?
The parents of a 4-year-old present to the pediatrician because they are concerned about the poor growth and odd behavior of their son. Their son has been at the 10th percentile for growth since birth and they have noticed that his skin seems to have a bluish hue to it whenever he cries or is agitated. Recently, they have noticed that when he squats it seems to relieve these symptoms. What was the embryologic cause of this patient's current symptoms?
A newborn is rushed to the neonatal ICU after becoming cyanotic shortly after birth. An ultrasound is performed which shows the aorta coming off the right ventricle and lying anterior to the pulmonary artery. The newborn is given prostaglandin E1 and surgery is planned to correct the anatomic defect. Which of the following developmental processes failed to occur in the newborn?
A 5-day-old boy is brought to the emergency department by his mother because of a 2-day history of difficulty feeding and multiple episodes of his lips turning blue. He was born at home via spontaneous vaginal delivery and Apgar scores were 7 and 8 at 1 and 5 minutes, respectively. Physical examination shows grunting and moderate intercostal and subcostal retractions. Echocardiography shows a single vessel exiting from the heart. Which of the following is the most likely underlying cause of this patient's condition?
A patient in the neonatal intensive care unit develops severe cyanosis. Cardiac exam reveals a single loud S2 with a right ventricular heave. Echocardiography reveals an aorta lying anterior and right of the pulmonary artery. Which of the following processes failed during fetal development?
Practice by Chapter
Primitive heart tube formation
Practice Questions
Cardiac looping
Practice Questions
Atrial septation
Practice Questions
Ventricular septation
Practice Questions
Outflow tract septation
Practice Questions
Valve development
Practice Questions
Cardiac conduction system development
Practice Questions
Coronary vasculature development
Practice Questions
Fetal circulation
Practice Questions
Congenital heart defects
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app