
Head & Neck — MCQs

On this page
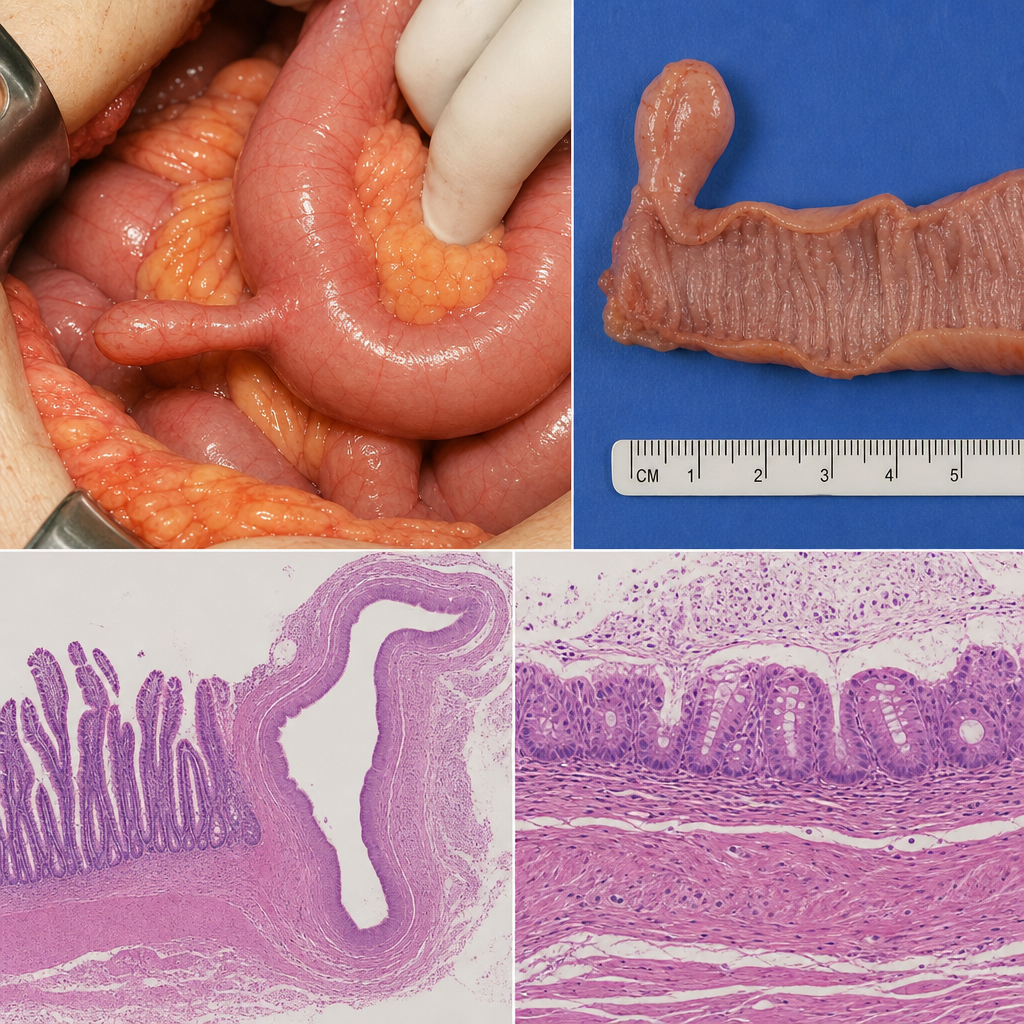
During a routine appendectomy in a 19-year-old man, the surgeon identifies a 5 cm blind-ended diverticulum on the antimesenteric border of the ileum, approximately 60 cm proximal to the ileocecal valve. Histological examination of the resected specimen reveals heterotopic gastric mucosa within the diverticulum wall alongside normal ileal mucosa and a well-defined muscularis propria continuous with the bowel wall. Which developmental structure failed to obliterate to produce this anomaly?
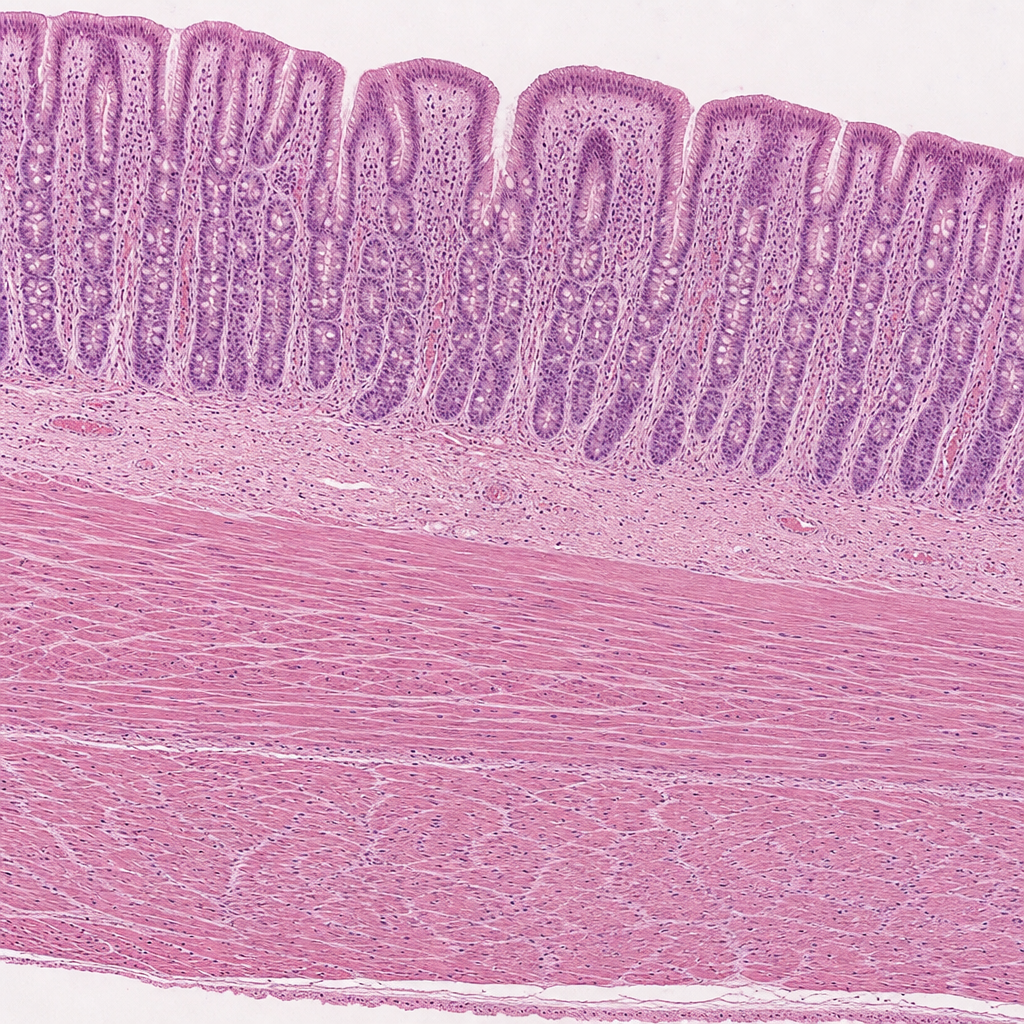
A histology slide from a routine autopsy is shown. The image reveals a tubular structure whose wall contains an inner oblique, middle circular, and outer longitudinal smooth muscle layer. The mucosa is lined by simple columnar epithelium with prominent gastric pits, and the lamina propria contains straight tubular glands extending the full depth of the mucosa with parietal (oxyntic) cells and chief cells that open into the base of the pits. The submucosa is unremarkable. Which region of the gastrointestinal tract does this specimen most likely represent?
Impaired gag reflex is seen due to a lesion in which cranial nerves?
Which tongue papillae do not have taste buds?
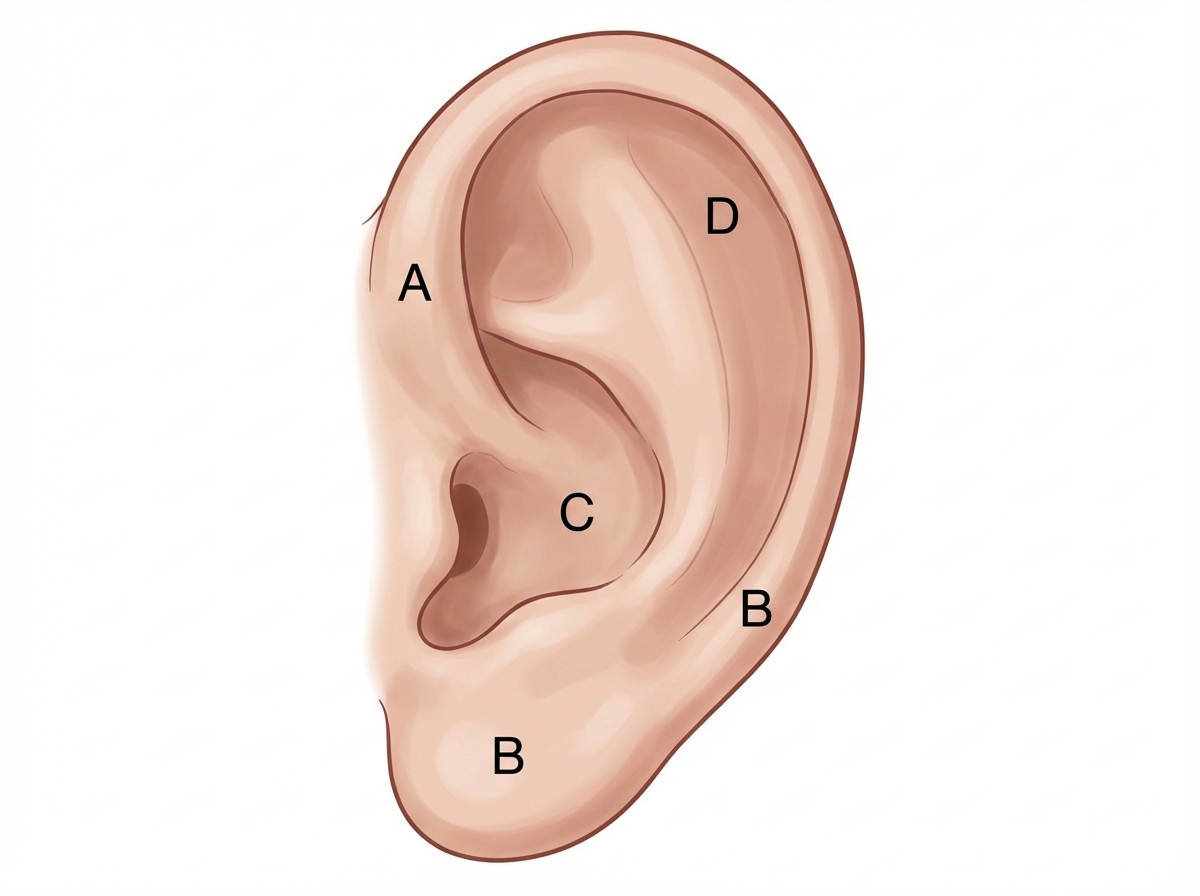
Match the following nerves to their respective areas of supply to the auricle
Practice by Chapter
Skull and cranial cavity
Practice Questions
Face and scalp
Practice Questions
Orbital structures
Practice Questions
Ear anatomy and vestibular system
Practice Questions
Nasal cavity and paranasal sinuses
Practice Questions
Oral cavity and pharynx
Practice Questions
Larynx and vocal apparatus
Practice Questions
Triangles of the neck
Practice Questions
Deep structures of the neck
Practice Questions
Cranial nerves and their pathways
Practice Questions
Cervical sympathetic chain
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app