
Gross Anatomy — MCQs

On this page
A 22-year-old Caucasian male is stabbed in his left flank, injuring his left kidney. As the surgeon undertakes operative repair, she reviews relevant renal anatomy. All of the following are correct regarding the left kidney EXCEPT?
A 21-year-old man was involved in a motor vehicle accident and died. At autopsy, the patient demonstrated abnormally increased mobility at the neck. A section of cervical spinal cord at C6 was removed and processed into slides. Which of the following gross anatomic features is most likely true of this spinal cord level?
A 65-year-old woman with osteoarthritis comes to the physician because of severe lower back and left leg pain. She has chronic lower back pain that is usually well-controlled with ibuprofen, but 3 hours ago her back pain acutely worsened after she picked up her 3-year-old granddaughter. The pain radiates from her lower back over her left outer thigh and knee towards the top of her big toe. Physical examination shows a diminished Achilles reflex on the left side. Muscle strength is 5/5 in all extremities and there are no sensory deficits. Steroid injection into which of the following anatomical locations is most likely to relieve her symptoms?
A 17-year-old boy is brought to the pediatrician by his mother for fatigue. The patient reports that he was supposed to try out for winter track this year, but he had to quit because his “legs just give up.” He also reports increased difficulty breathing with exercise but denies chest pain or palpitations. He has no chronic medical conditions and takes no medications. He has had no surgeries in the past. The mother reports that he met all his pediatric milestones and is an “average” student. He is up-to-date on all childhood vaccinations, including a recent flu vaccine. On physical examination, there is mild lumbar lordosis. The patient’s thighs appear thin in diameter compared to his lower leg muscles, and he walks on his toes. An electrocardiogram shows 1st degree atrioventricular nodal block. Which of the following is the most likely cause of the patient’s condition?
A 17-year-old boy is brought to the emergency department by his parents because of crushing chest pain, nausea, and vomiting for the past 2 hours. The pain is constant and radiates to his left shoulder. Over the past year, he has been admitted to the hospital twice for deep vein thrombosis. He has a history of learning disability and has been held back three grades. The patient is at the 99th percentile for length and the 45th percentile for weight. His pulse is 110/min, respirations are 21/min, and blood pressure is 128/84 mm Hg. His fingers are long and slender, and his arm span exceeds his body height. Electrocardiography shows ST-segment elevation in leads V1 and V2. His serum troponin I concentration is 2.0 ng/mL (N ≤ 0.04). Coronary angiography shows 90% occlusion of the proximal left anterior descending artery. Further evaluation of this patient is most likely to show which of the following findings?
A morbidly obese 43-year-old man presents for elective bariatric surgery after previously failing several non-surgical weight loss plans. After discussing the risks and benefits of several different procedures, a sleeve gastrectomy is performed. During the surgery, the surgeon begins by incising into the right half of the greater curvature of the stomach. Which of the following arteries most likely directly provides the blood supply to this region of the stomach?
A 24-year-old woman comes to the emergency department because of abdominal pain, fever, nausea, and vomiting for 12 hours. Her abdominal pain was initially dull and diffuse but has progressed to a sharp pain on the lower right side. Two years ago she had to undergo right salpingo-oophorectomy after an ectopic pregnancy. Her temperature is 38.7°C (101.7°F). Physical examination shows severe right lower quadrant tenderness with rebound tenderness; bowel sounds are decreased. Laboratory studies show leukocytosis with left shift. An abdominal CT scan shows a distended, edematous appendix. The patient is taken to the operating room for an appendectomy. During the surgery, the adhesions from the patient's previous surgery make it difficult for the resident physician to identify the appendix. Her attending mentions that she should use a certain structure for guidance to locate the appendix. The attending is most likely referring to which of the following structures?
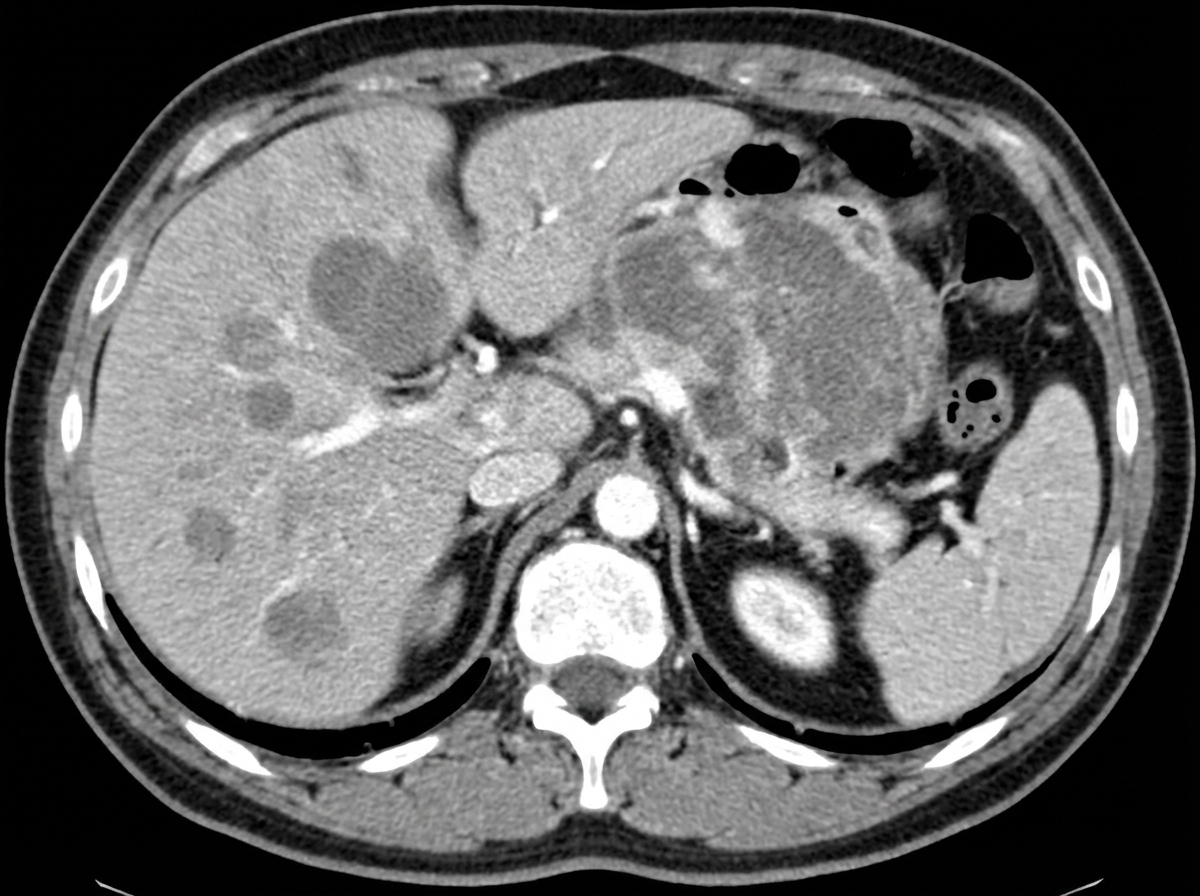
A 40-year-old man presents with severe fatigue, dyspnea on exertion, and weight loss. He reports a weight loss of 15 kg (33.0 lb) over the past 3 months and feels full almost immediately after starting to eat, often feeling nauseous and occasionally vomiting. He also reports passing black, tarry stools for the past week. Past medical history is not significant. However, the patient reports a 10-pack-year smoking history. His temperature is 37.0°C (98.6°F), respiratory rate is 15/min, pulse is 67/min, and blood pressure is 122/98 mm Hg. Physical examination reveals paleness and conjunctival pallor. Abdominal examination reveals an ill-defined nontender mass in the epigastric region along with significant hepatomegaly. Routine laboratory studies show a hemoglobin level of 7.2 g/dL. A contrast CT scan of the abdomen is presented below, revealing a mass in the stomach proximal to the duodenojejunal junction. Which anatomical landmark is used to classify this patient's gastrointestinal bleeding as upper versus lower GI bleeding?
A 49-year-old man comes to the physician because of severe, shooting pain in his lower back for the past 2 weeks. The pain radiates down the back of both legs and started after he lifted a concrete manhole cover from the ground. Physical examination shows decreased sensation to light touch bilaterally over the lateral thigh area and lateral calf bilaterally. Patellar reflex is decreased on both sides. The passive raising of either the right or left leg beyond 30 degrees triggers a shooting pain down the leg past the knee. Which of the following is the most likely underlying cause of this patient's current condition?
Practice by Chapter
Anatomical terminology and positions
Practice Questions
Fascial planes and compartments
Practice Questions
Musculoskeletal system overview
Practice Questions
Cardiovascular system overview
Practice Questions
Respiratory system overview
Practice Questions
Digestive system overview
Practice Questions
Urinary system overview
Practice Questions
Reproductive system overview
Practice Questions
Integumentary system
Practice Questions
Anatomical variations and clinical significance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app