
Anatomical terminology and positions — MCQs

A 17-year-old boy comes to the physician because of a 3-month history of pain in his right shoulder. He reports that he has stopped playing for his high school football team because of persistent difficulty lifting his right arm. Physical examination shows impaired active abduction of the right arm from 0 to 15 degrees. After passive abduction of the right arm to 15 degrees, the patient is able to raise his arm above his head. The dysfunctional muscle in this patient is most likely to be innervated by which of the following nerves?
A neurology resident sees a stroke patient on the wards. This 57-year-old man presented to the emergency department after sudden paralysis of his right side. He was started on tissue plasminogen activator within 4 hours, as his wife noticed the symptoms and immediately called 911. When the resident asks the patient how he is doing, he replies by saying that his apartment is on Main St. He does not seem to appropriately answer the questions being asked, but rather speaks off topic. He is able to repeat the word "fan." His consciousness is intact, and his muscle tone and reflexes are normal. Upon striking the lateral part of his sole, his big toe extends upward and the other toes fan out. Which of the following is the area most likely affected in his condition?
A patient undergoes spinal surgery at the L4-L5 level. During the procedure, which of the following ligaments must be divided first to access the spinal canal?
A 40-year-old male presents to the physician's office complaining of an inability to push doors open. He has had this problem since he was playing football with his children and was tackled underneath his right arm on his lateral chest. On examination, he has a winged scapula on the right side. Which of the following nerves is most likely the cause of this presentation?
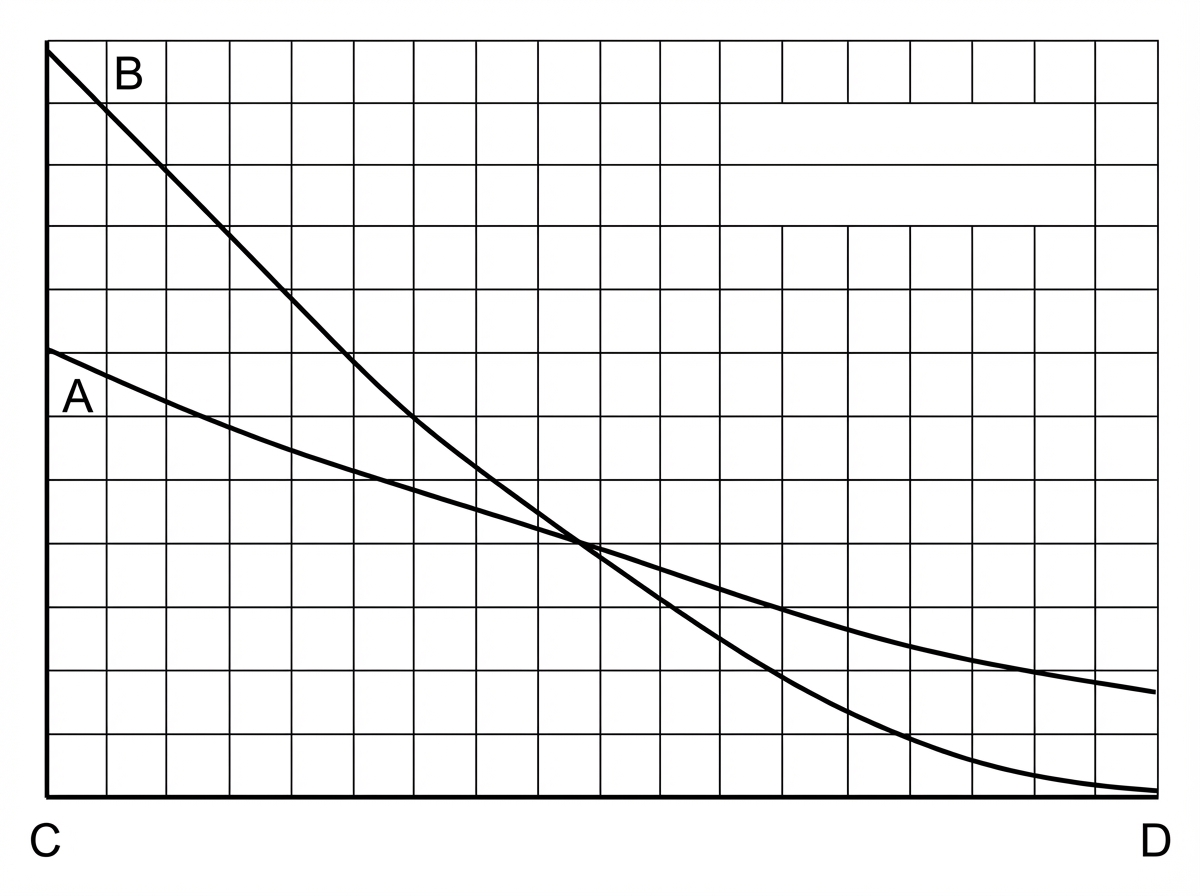
A young researcher is responsible for graphing laboratory data involving pulmonary blood flow and ventilation pattern obtained from a healthy volunteer who was standing in an upright position. After plotting the following graph, the researcher realizes he forgot to label the curves and the x-axis (which represents the position in the lung). Which of the following is the appropriate label for each point on the graph?
An MRI of a patient with low back pain reveals compression of the L5 nerve root. Which of the following muscles would most likely show weakness during physical examination?
A 24-year-old woman comes to the emergency department because of abdominal pain, fever, nausea, and vomiting for 12 hours. Her abdominal pain was initially dull and diffuse but has progressed to a sharp pain on the lower right side. Two years ago she had to undergo right salpingo-oophorectomy after an ectopic pregnancy. Her temperature is 38.7°C (101.7°F). Physical examination shows severe right lower quadrant tenderness with rebound tenderness; bowel sounds are decreased. Laboratory studies show leukocytosis with left shift. An abdominal CT scan shows a distended, edematous appendix. The patient is taken to the operating room for an appendectomy. During the surgery, the adhesions from the patient's previous surgery make it difficult for the resident physician to identify the appendix. Her attending mentions that she should use a certain structure for guidance to locate the appendix. The attending is most likely referring to which of the following structures?
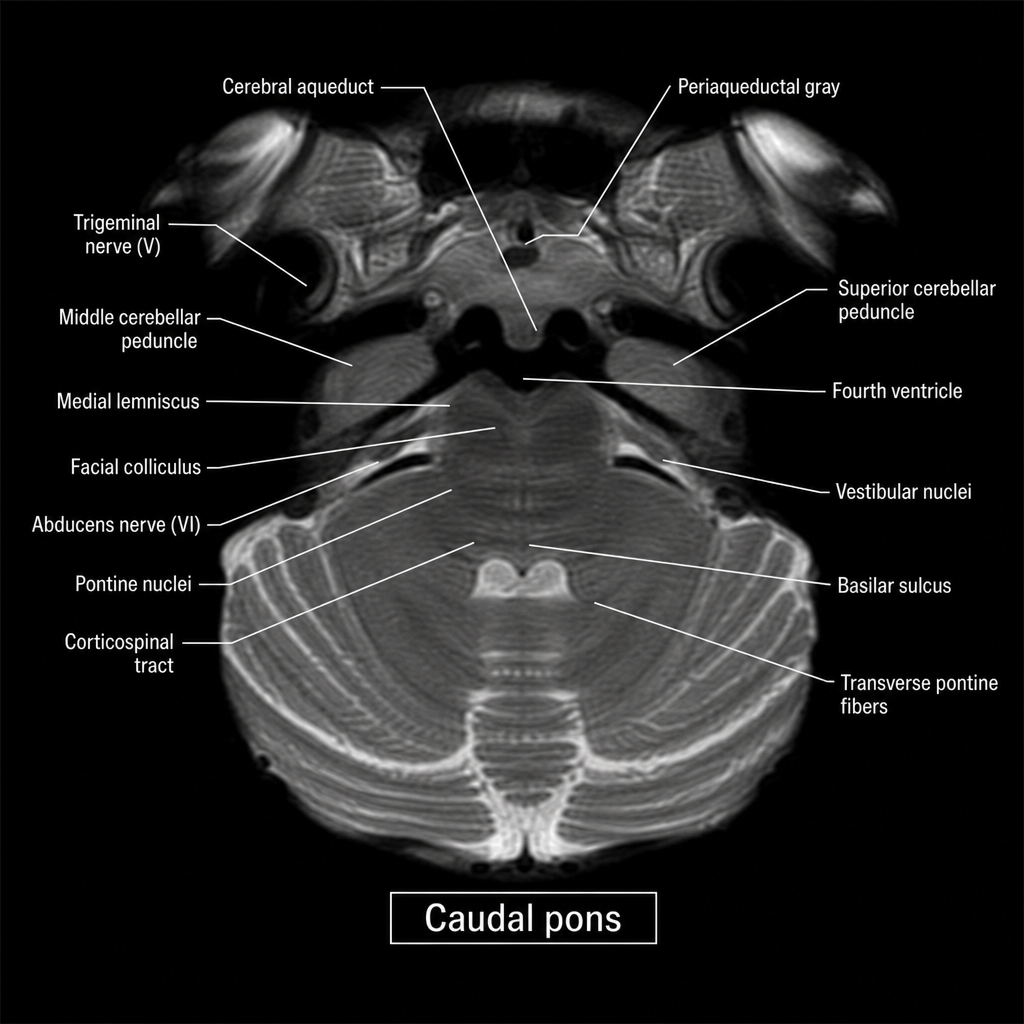
An axial MRI section through the brainstem is shown at the level indicated by the label 'caudal pons.' A 67-year-old man with hypertension presents with acute-onset left facial weakness involving the upper and lower face, left lateral gaze palsy, and right-sided limb weakness with an extensor plantar response on the right. The lesion responsible for all of these findings is most likely located in which region of the image?
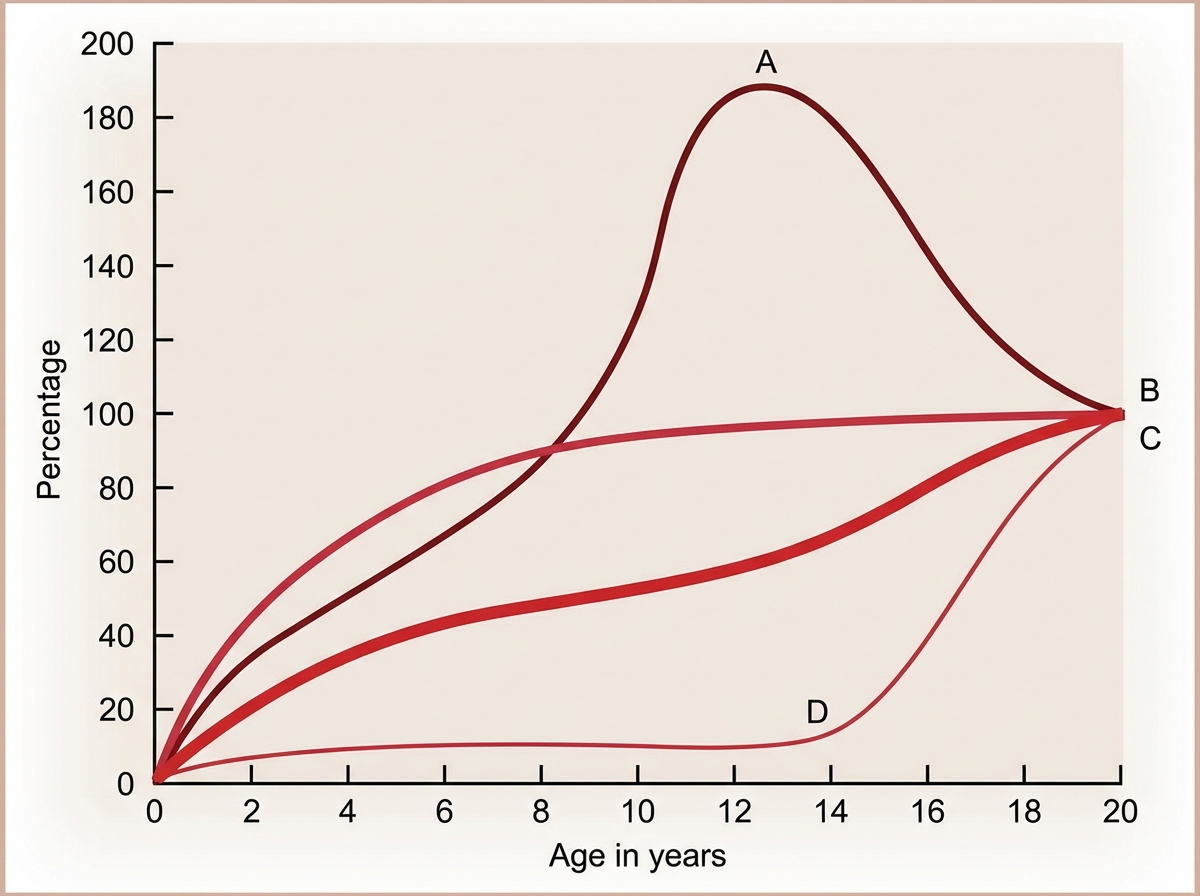
The Image shows the growth curve of different organs with age. Identify A in the graph.
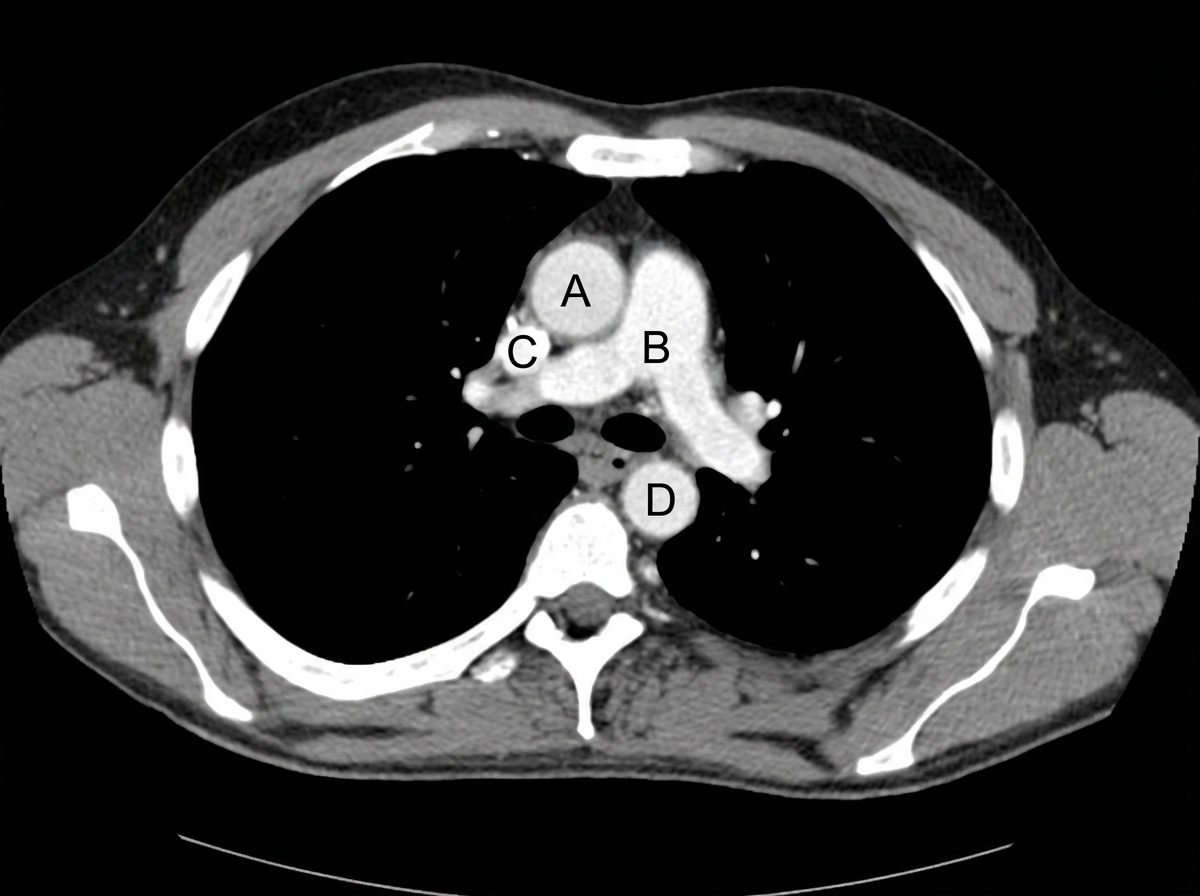
Identify the labeled structures correctly in the axial CT image of the thorax
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app