
Gross Anatomy — MCQs

On this page
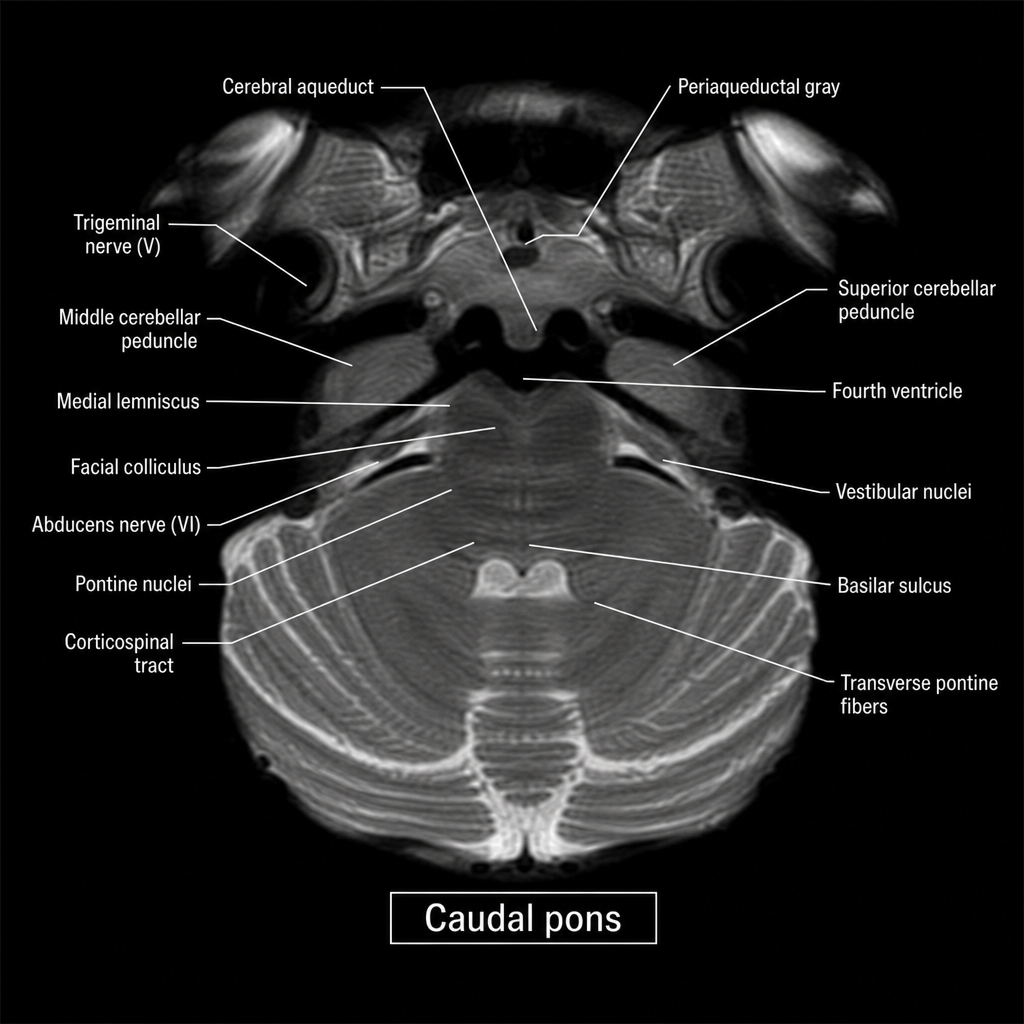
An axial MRI section through the brainstem is shown at the level indicated by the label 'caudal pons.' A 67-year-old man with hypertension presents with acute-onset left facial weakness involving the upper and lower face, left lateral gaze palsy, and right-sided limb weakness with an extensor plantar response on the right. The lesion responsible for all of these findings is most likely located in which region of the image?
Practice by Chapter
Anatomical terminology and positions
Practice Questions
Fascial planes and compartments
Practice Questions
Musculoskeletal system overview
Practice Questions
Cardiovascular system overview
Practice Questions
Respiratory system overview
Practice Questions
Digestive system overview
Practice Questions
Urinary system overview
Practice Questions
Reproductive system overview
Practice Questions
Integumentary system
Practice Questions
Anatomical variations and clinical significance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app