
GI development — MCQs

On this page
A newborn presents with bilious vomiting 24 hours after birth. Physical examination reveals a distended upper abdomen and a scaphoid lower abdomen. An abdominal radiograph shows a 'double bubble' sign with no distal gas. The infant has Down syndrome. Apply your knowledge of embryology to identify the most likely anatomical basis for this condition.
A 3-day-old newborn is brought to the physician because of abdominal distention, inconsolable crying, and 3 episodes of bilious vomiting since the previous evening. He was delivered at home at 40 weeks' gestation by a trained midwife. He has not passed meconium. Physical examination shows abdominal distention, a tight anal sphincter, and an explosive passage of air and feces on removal of the examining finger. Abnormal development of which of the following best explains this patient's condition?
A 60-year-old gentleman passes away after a car accident. On routine autopsy it is incidentally noted that he has both a ventral and dorsal pancreatic duct. This incidental finding observed by the pathologist is generated due to failure of which of the following embryological processes?
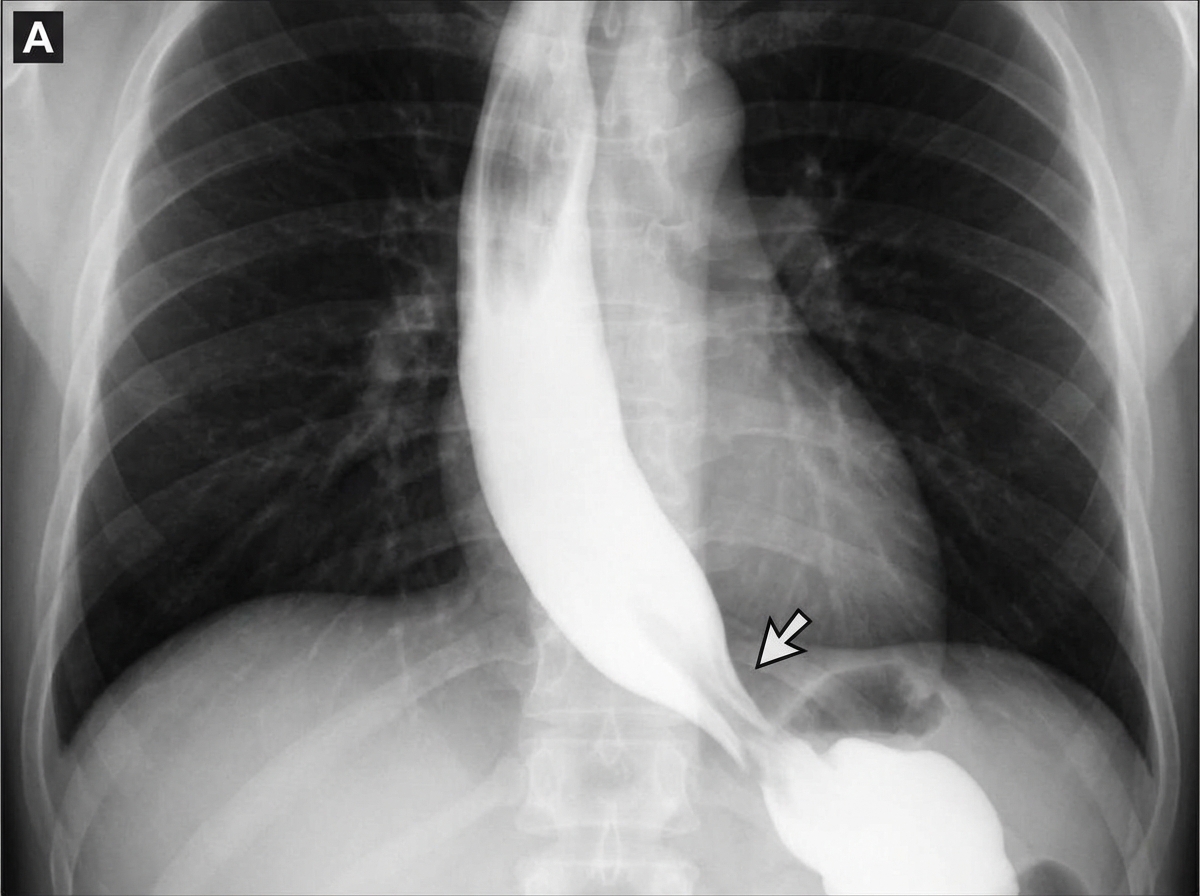
A 45-year-old woman comes to the physician because of progressive difficulty swallowing solids and liquids over the past 4 months. She has lost 4 kg (9 lb) during this period. There is no history of serious illness. She emigrated to the US from Panama 7 years ago. She does not smoke cigarettes or drink alcohol. Cardiopulmonary examination shows a systolic murmur and an S3 gallop. A barium radiograph of the chest is shown. Histopathologic examination of the esophageal wall is most likely to show which of the following?
A 3-month-old boy has a malodorous umbilical discharge that developed shortly after umbilical cord separation. He was treated for omphalitis with 3 doses of antibiotics. The vital signs are as follows: blood pressure 70/40 mm Hg, heart rate 125/min, respiratory rate 34/min, and temperature 36.8℃ (98.2℉). On physical examination, he appears active and well-nourished. The skin in the periumbilical region is red and macerated. There is a slight green-yellow discharge from the umbilicus which resembles feces. The remnant of which structure is most likely causing the patient’s symptoms?
An otherwise healthy 1-month-old girl is brought to the physician because of a 1-day history of multiple episodes of bilious vomiting. She is diagnosed with intestinal malrotation and volvulus and undergoes emergency laparotomy. During surgery, a 3 x 3 cm cystic mass is excised from behind the umbilicus. Microscopic examination of the mass shows mature nonciliated columnar epithelium with some goblet cells lining the inner cyst wall. Dilation of which of the following structures is the most likely cause of this patient's mass?
A new mother expresses her concerns because her 1-day-old newborn has been having feeding difficulties. The child vomits after every feeding and has had a continuous cough since shortly after birth. The mother denies any greenish coloration of the vomit and says that it is only composed of whitish milk that the baby just had. The child exhibits these coughing spells during the exam, at which time the physician notices the child’s skin becoming cyanotic. The mother states that the child was born vaginally with no complications, although her records show that she had polyhydramnios during her last ultrasound before the delivery. Which of the following is the most likely cause of the patient’s symptoms?
Practice by Chapter
Primitive gut formation
Practice Questions
Foregut development and derivatives
Practice Questions
Midgut development and rotation
Practice Questions
Hindgut development
Practice Questions
Liver and biliary system development
Practice Questions
Pancreas development
Practice Questions
Spleen development
Practice Questions
Abdominal wall development
Practice Questions
Diaphragm development
Practice Questions
Congenital anomalies of GI tract
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app