
GI development — MCQs

On this page
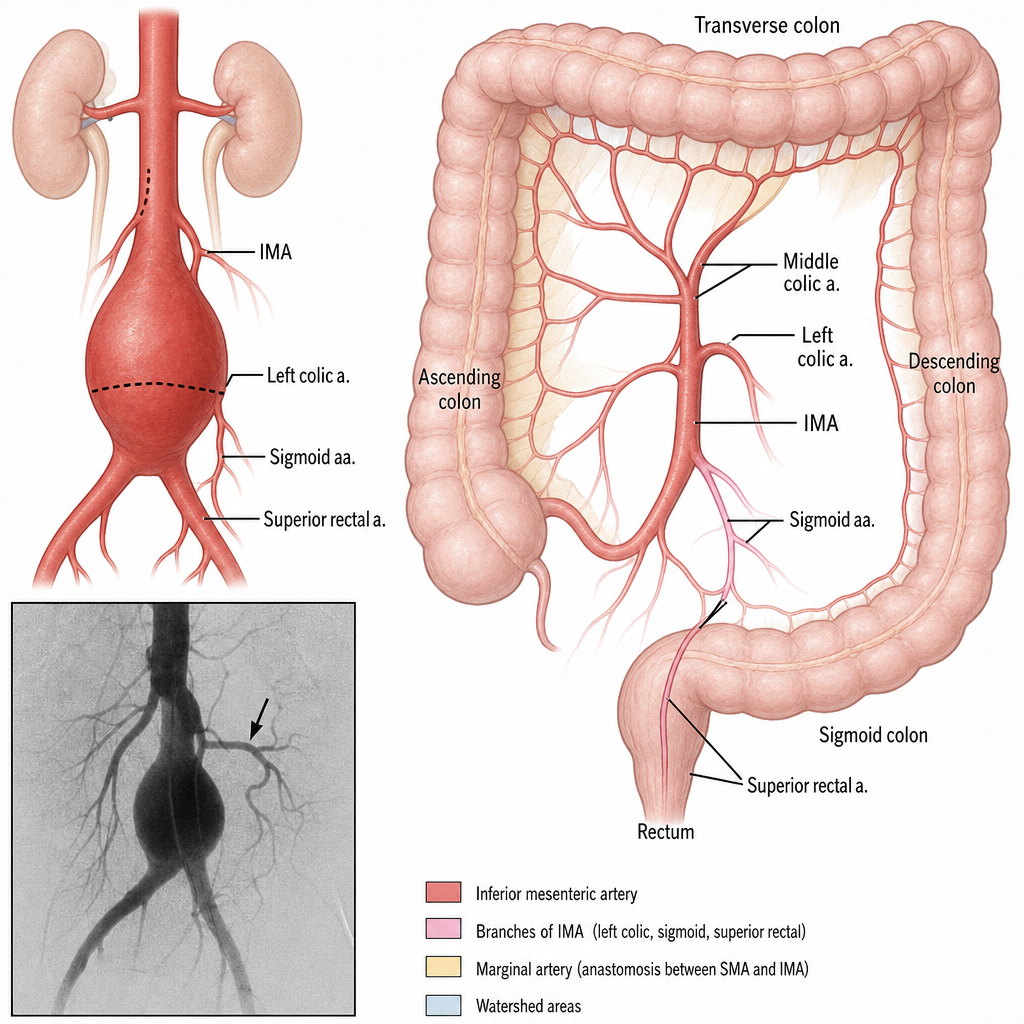
A vascular surgery team is reviewing pre-operative angiography for a 67-year-old man with a large abdominal aortic aneurysm extending to the bifurcation. The aneurysm sac and the origin of the inferior mesenteric artery (IMA) have been identified on imaging. The surgeon notes that the IMA must be reimplanted to preserve blood supply to a critical region. Based on the vascular territory of the IMA and its anastomotic connections, which clinical consequence is the surgical team most concerned about preventing if the IMA is ligated without reimplantation and collateral flow via the marginal artery of Drummond is inadequate?
A 4-week-old infant presents with progressively worsening jaundice. Laboratory studies show direct hyperbilirubinemia, elevated gamma-glutamyl transferase, and pale stools. Liver biopsy shows bile duct proliferation and portal fibrosis. Intraoperative cholangiogram reveals absence of extrahepatic bile ducts with normal intrahepatic ducts proximally. The gallbladder is present but atretic. Synthesize the embryological timing and pathophysiological mechanism of this postnatal progressive condition.
A newborn presents with respiratory distress immediately after birth. Chest radiograph shows bowel loops in the left hemithorax with mediastinal shift to the right and hypoplastic left lung. The infant has scaphoid abdomen. During fetal ultrasound at 9 weeks, normal diaphragm development was noted, but at 20 weeks, abdominal contents were seen in the chest. Evaluate the critical developmental period and mechanism of lung hypoplasia.
A 2-year-old child presents with painless rectal bleeding. A Meckel scan using technetium-99m pertechnetate shows increased uptake in the right lower quadrant, 60 cm from the ileocecal valve. At surgery, a 5 cm diverticulum is found on the antimesenteric border containing heterotopic gastric mucosa. Evaluate the embryological remnant and the developmental principle explaining the heterotopic tissue.
An infant presents with drooling, coughing with feeds, and inability to pass a nasogastric tube beyond 10 cm. Chest radiograph shows the NG tube coiled in the upper esophagus and gas in the stomach and bowel. Bronchoscopy reveals a fistula between the distal esophagus and trachea. Analyze the embryological partitioning defect that produced this most common variant.
A newborn is found to have a portion of bowel protruding through the umbilical ring, covered by a membrane consisting of amnion and peritoneum. The liver is not herniated. Prenatal ultrasound at 10 weeks showed normal physiologic herniation of the midgut. Analyze the developmental timing that led to this condition versus normal development.
A 6-hour-old neonate develops bilious vomiting and bloody stools. Abdominal examination reveals peritonitis and the infant is tachycardic. Upper GI series shows the duodenojejunal junction to the right of midline and the cecum in the right upper quadrant. At surgery, the entire midgut is twisted clockwise around the superior mesenteric artery. Analyze the embryological sequence that predisposed to this acute condition.
A 2-day-old infant presents with abdominal distension and failure to pass meconium. Abdominal radiograph shows dilated loops of bowel. A rectal suction biopsy is performed and shows absence of ganglion cells in the submucosal and myenteric plexuses. Apply developmental principles to determine the underlying embryological defect.
A newborn female is noted to have meconium passing through the vagina. Further evaluation reveals a fistulous connection between the rectum and the vaginal vestibule. The infant has normal anal opening but an imperforate high vaginal tract. Apply your understanding of cloaca division to identify the embryological defect.
A 3-week-old male infant presents with progressive projectile non-bilious vomiting after feeding. On examination, an olive-shaped mass is palpable in the right upper quadrant. Laboratory studies show hypochloremic, hypokalemic metabolic alkalosis. Apply embryological principles to determine which developmental structure is affected.
Practice by Chapter
Primitive gut formation
Practice Questions
Foregut development and derivatives
Practice Questions
Midgut development and rotation
Practice Questions
Hindgut development
Practice Questions
Liver and biliary system development
Practice Questions
Pancreas development
Practice Questions
Spleen development
Practice Questions
Abdominal wall development
Practice Questions
Diaphragm development
Practice Questions
Congenital anomalies of GI tract
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app