
Embryology — MCQs

On this page
A 3175-g (7-lb) male newborn is delivered at 39 weeks' gestation to a 29-year-old primigravid woman following a spontaneous vaginal delivery. Apgar scores are 8 and 9 at 1 and 5 minutes, respectively. Cardiac examination in the delivery room shows a continuous machine-like murmur. An echocardiogram shows a structure with blood flow between the pulmonary artery and the aorta. This structure is most likely a derivate of which of the following?
A researcher is studying the brains of patients who recently died from stroke-related causes. One specimen has a large thrombus in an area of the brain that is important in relaying many modalities of sensory information from the periphery to the sensory cortex. Which of the following embryologic structures gave rise to the part of the brain in question?
An 11-year-old girl is brought to the office by her mother due to complaint of intermittent and severe periumbilical pain for 1 day. She does not have any significant past medical history. She provides a history of a recent school trip to the suburbs. On physical examination, there is a mild tenderness around the umbilicus without any distension or discharge. There is no rebound tenderness. Bowel sounds are normal. An abdominal imaging shows enlarged mesenteric lymph nodes, and she is diagnosed with mesenteric lymphadenitis. However, incidentally, a mass of tissue was seen joining the inferior pole of both kidneys as shown in the image. Which of the following best describes this renal anomaly?

A 2-day-old infant dies of severe respiratory distress following a gestation complicated by persistent oligohydramnios. Upon examination at autopsy, the left kidney is noted to selectively lack cortical and medullary collecting ducts. From which of the following embryological structures do the cortical and medullary collecting ducts arise?
A 23-year-old woman, gravida 2, para 1, at 26 weeks gestation comes to the physician for a routine prenatal visit. Physical examination shows a uterus consistent in size with a 26-week gestation. Fetal ultrasonography shows a male fetus with a thick band constricting the right lower arm; the limb distal to the constrictive band cannot be visualized. The most likely condition is an example of which of the following embryological abnormalities?
A 35-year-old G2P1 delivers a boy in the 40th week of gestation. The pregnancy was uncomplicated. The newborn had Apgar scores of 7 and 9 at the 1st and 5th minutes, respectively. On physical examination, the newborn is noted to have a left-sided cleft lip. The hard palate and nose are normal. Which of the following statements describes the cause of the abnormality?
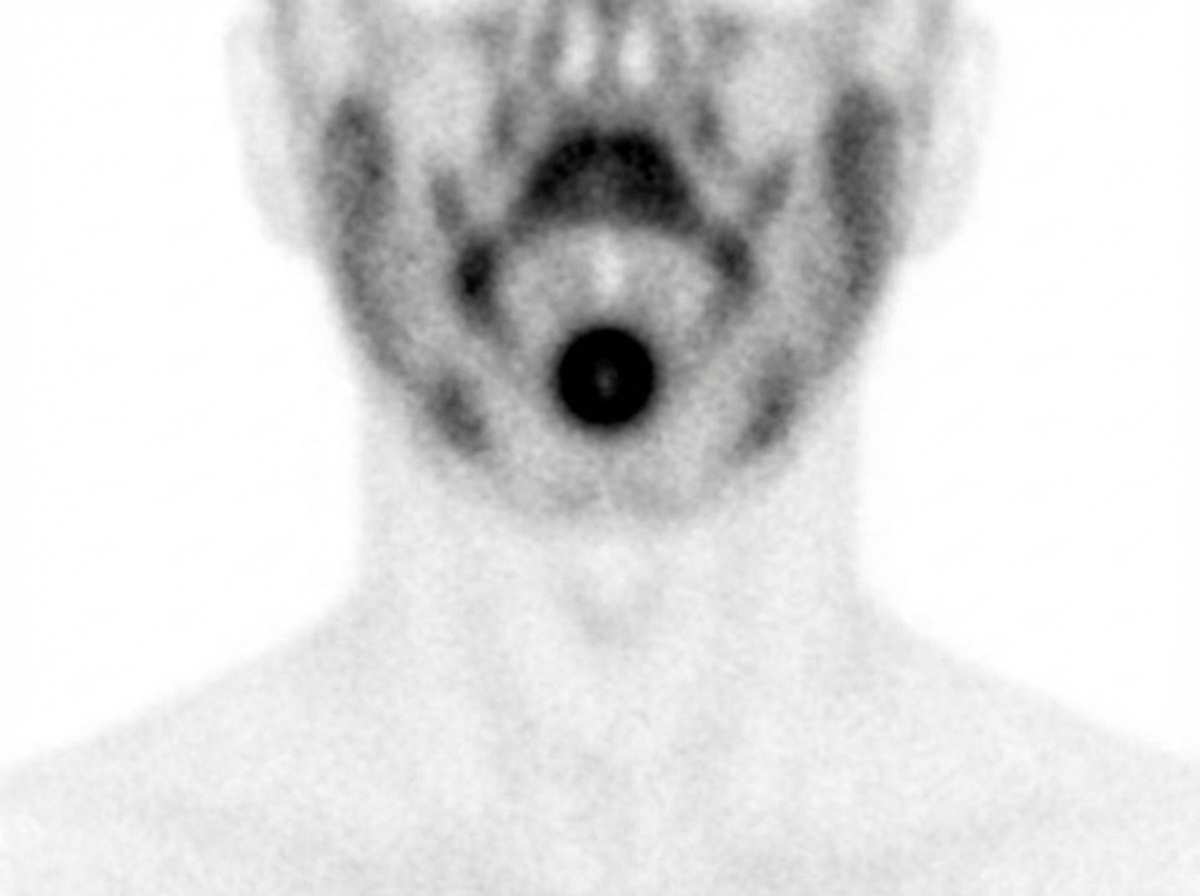
A 16-year-old boy comes to the physician because of a 1-week history of difficulty swallowing, a foreign body sensation at the back of his throat, and trouble breathing at night. He has just recovered from an upper respiratory tract infection that began 5 days ago. On questioning, he reports that he has had similar symptoms in the past each time he has had an upper respiratory tract infection. Physical examination shows a 3 x 2-cm, nontender, rubbery midline mass at the base of the tongue. His skin is dry and cool. An image of his technetium-99m pertechnetate scan is shown. Which of the following is the most likely underlying cause of this patient’s condition?
A 31-year-old G2P2 female at 40 weeks gestation presents to the hospital following a rush of water that came from her vagina. She is 4 cm dilated and 80% effaced. Fetal heart tracing shows a pulse of 155/min with variable decelerations. About 12 hours after presentation, she gives birth to a 6 lb 15 oz baby boy with APGAR scores of 8 and 9 at 1 and 5 minutes, respectively. Which of the following structures is responsible for inhibition of female internal genitalia?
A 23-year-old man comes to the physician for evaluation of decreased hearing, dizziness, and ringing in his right ear for the past 6 months. Physical examination shows multiple soft, yellow plaques and papules on his arms, chest, and back. There is sensorineural hearing loss and weakness of facial muscles bilaterally. His gait is unsteady. An MRI of the brain shows a 3-cm mass near the right internal auditory meatus and a 2-cm mass at the left cerebellopontine angle. The abnormal cells in these masses are most likely derived from which of the following embryological structures?
Practice by Chapter
Gametogenesis
Practice Questions
Fertilization and zygote formation
Practice Questions
Cleavage and blastocyst formation
Practice Questions
Implantation
Practice Questions
Bilaminar and trilaminar disc formation
Practice Questions
Neurulation and neural tube development
Practice Questions
Somite formation and derivatives
Practice Questions
Placenta and fetal membranes
Practice Questions
Limb development
Practice Questions
Urogenital system development
Practice Questions
Teratogens and critical periods
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app