
Embryology — MCQs

On this page
A 7-year-old boy presents with difficulty swallowing, diarrhea, itching, and weakness. He also complains of episodes of headaches, sweating, and palpitations, which are accompanied by fear and tend to end with micturition. His mother is concerned about the strange nodules on his lips and eyelids. The boy's younger brother had similar nodules and died at 10 years of age of unknown causes. The patient’s vital signs are as follows: blood pressure 130/80 mm Hg, heart rate 107/min, respiratory rate 14/min, and temperature 36.9℃ (98.4℉). The child is tall, thin, has disproportionately long arms and legs, and increased thoracic spine kyphosis. There are multiple yellow-white, sessile, painless nodules on the patient’s lips, and buccal and eyelid mucosa. There is a painless lump in the area of the left thyroid lobe and enlargement of the posterior cervical lymph nodes on the left side. What is the most probable embryonic origin of the cells in the lump?
A 17-year old girl is brought to the physician by her mother because menarche has not yet occurred. She is at the 3rd percentile for height. Examination of a buccal mucosal scraping shows no Barr bodies. Karyotyping of a neutrophil shows 45 chromosomes. Which of the following is the most likely underlying cause of this patient's cytogenetic abnormality?
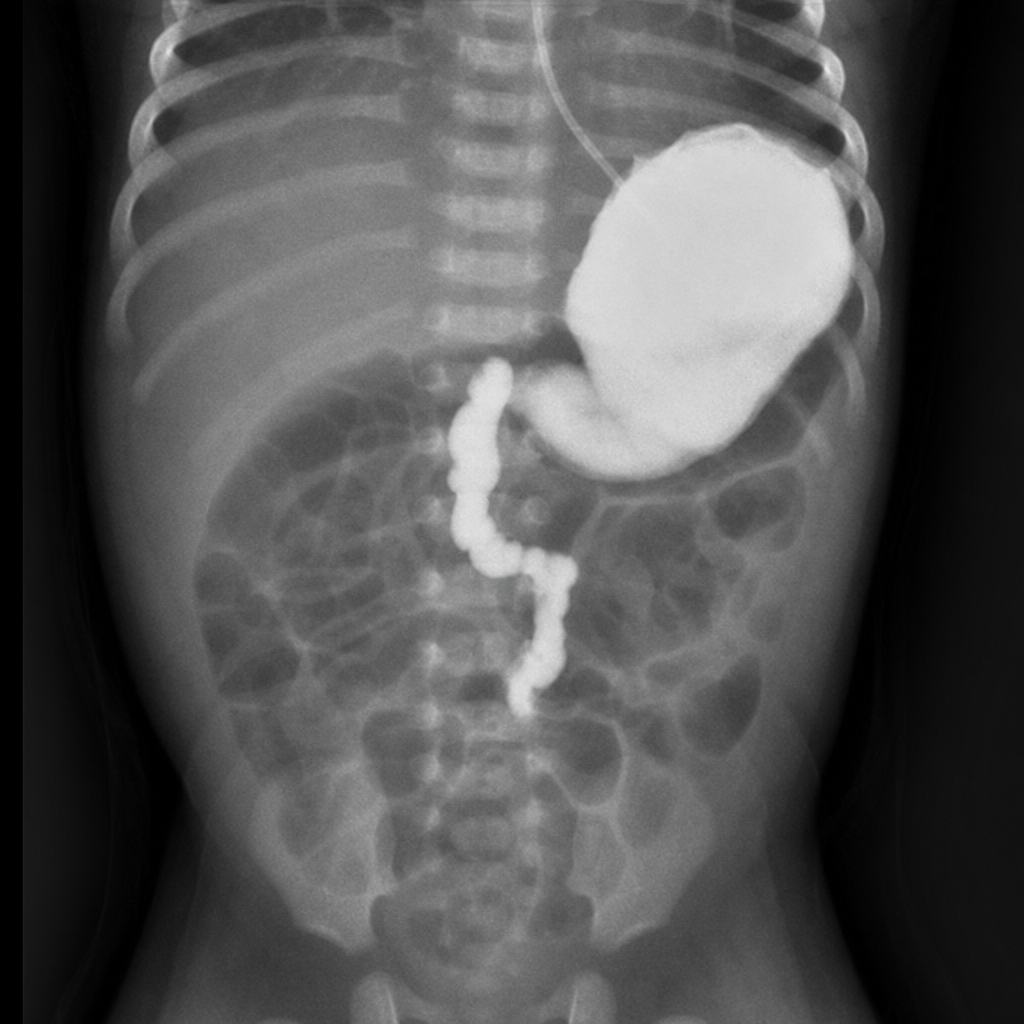
A 10-day-old male newborn is brought to the physician by his mother because of difficulty feeding and frequent nonbilious vomiting. His stool is soft and yellow-colored. The pregnancy was complicated by polyhydramnios and results from chorionic villus sampling showed a 47, XY, +21 karyotype. Physical examination shows mild abdominal distention and normal bowel sounds. An x-ray of the abdomen with oral contrast is shown, demonstrating a narrowed duodenal lumen with an intraluminal filling defect consistent with a duodenal web. The most likely cause of his condition is due to a defect in which of the following embryologic processes?
A 29-year-old woman comes to the physician because of poor balance and recurrent falls for the past month. She has also had blurry vision in her right eye for the past 2 weeks. She reports worsening of her symptoms after taking warm baths. Physical examination shows generalized hyperreflexia and an intention tremor. Romberg sign is positive. Visual acuity is 20/50 in the left eye and 20/100 in the right eye, and she is unable to distinguish red from green colors. The cells primarily affected by this patient's condition are most likely derived from which of the following embryologic structures?
A mother brings her 2-year-old son to the pediatrician following an episode of abdominal pain and bloody stool. The child has otherwise been healthy and growing normally. On physical exam, the patient is irritable with guarding of the right lower quadrant of the abdomen. Based on clinical suspicion, pertechnetate scintigraphy demonstrates increased uptake in the right lower abdomen. Which of the following embryologic structures is associated with this patient’s condition?
A 2-day-old boy fails to pass meconium for the first 48 hours of life. He was born at term to a healthy 19-year-old woman after an uncomplicated pregnancy. At birth, his weight was 3.9 kg (8.6 lb); at the time of presentation, he weighs 3.8 kg (8.4 lb). His vital signs are as follows: blood pressure 70/50 mm Hg, heart rate 130/min, respiratory rate 33/min, and temperature 37.0℃ (98.6℉). On physical examination, he is fussy and appears mildly dehydrated. Bowel sounds are active on auscultation. His abdomen is mildly distended and no masses can be identified on palpation. The patient’s anus is patent. An upper gastrointestinal study with oral contrast demonstrates normal anatomy. A lower gastrointestinal series with barium enema reveals a large amount of retained barium contrast within a dilated sigmoid colon and a normal appearing rectum. The barium solution retention persisted beyond 24 hours after administration. Which of the following best describes the cause of the patient’s symptoms?
A newborn male born prematurely at 33 weeks is noted to have mild dyspnea and difficulty with feeding. Examination reveals bounding peripheral radial pulses and a continuous 'machine-like' murmur. The patient is subsequently started on indomethacin. Which of the following is the embryologic origin of the structure most likely responsible for this patient's presentation?
A 35-year-old female presents to her gynecologist complaining of vaginal discomfort. She reports that over the past two weeks, she has developed dyspareunia and feels as if there is a mass on the external aspect of her vagina. She is sexually active in a monogamous relationship. On physical examination, there is a 2 cm unilateral erythematous swelling on the right side of the posterolateral labia minora. Which of the following embryologic precursors gives rise to the affected tissue in this patient?
A 4-week-old boy is brought to the emergency department with a 2-day history of projectile vomiting after feeding. His parents state that he is their firstborn child and that he was born healthy. He developed normally for several weeks but started to eat less 1 week ago. Physical exam reveals a small, round mass in the right upper quadrant of the abdomen close to the midline. The infant throws up in the emergency department, and the vomitus is observed to be watery with no traces of bile. Which of the following is associated with the most likely cause of this patient's symptoms?
An investigator is studying the effects of an antihypertensive drug during pregnancy. Follow-up studies show that the drug can adversely affect differentiation of the ureteric bud into its direct derivatives in fetuses exposed during the first trimester. Which of the following structures is most likely to develop incorrectly in the affected fetus?
Practice by Chapter
Gametogenesis
Practice Questions
Fertilization and zygote formation
Practice Questions
Cleavage and blastocyst formation
Practice Questions
Implantation
Practice Questions
Bilaminar and trilaminar disc formation
Practice Questions
Neurulation and neural tube development
Practice Questions
Somite formation and derivatives
Practice Questions
Placenta and fetal membranes
Practice Questions
Limb development
Practice Questions
Urogenital system development
Practice Questions
Teratogens and critical periods
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app