
Embryology — MCQs

On this page
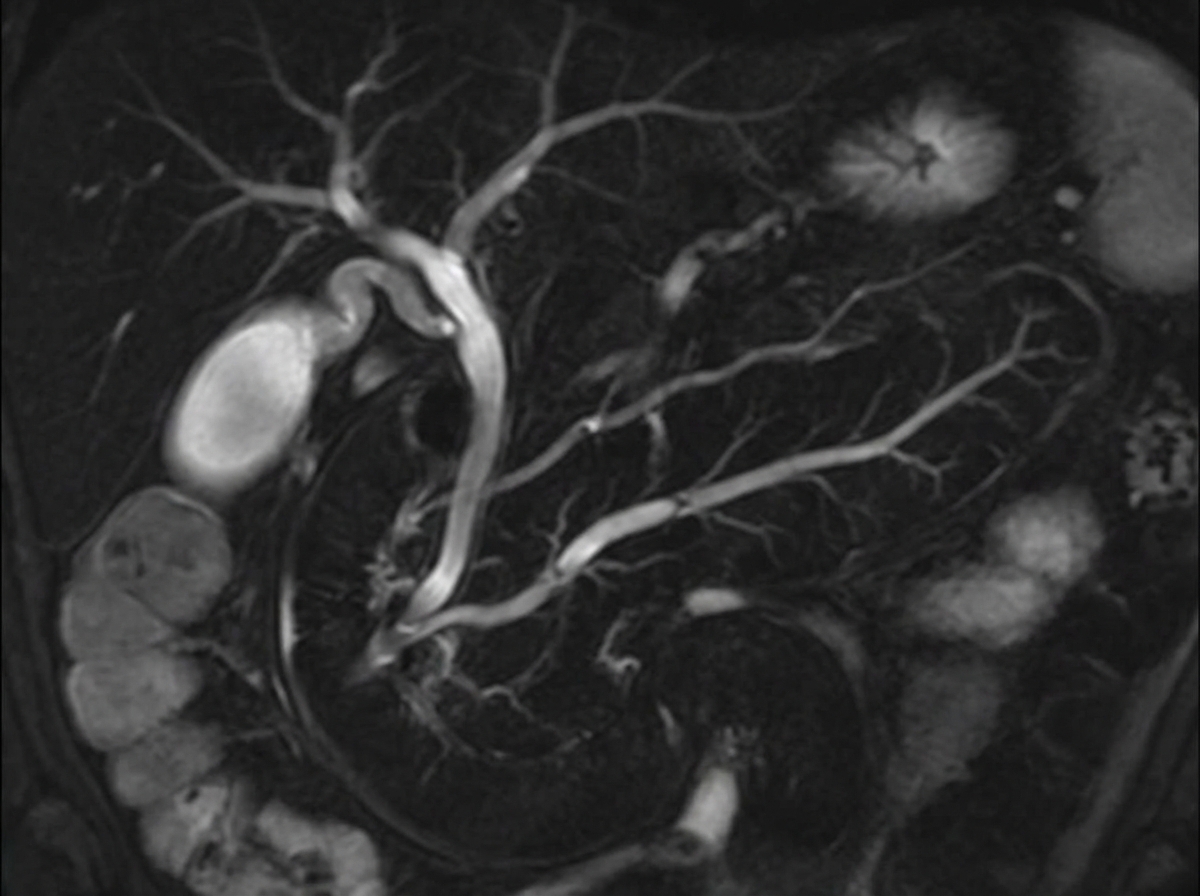
A 37-year-old man presents with dull, continuous epigastric pain that radiates to the back in a circumscribing fashion. The history is significant for 3 episodes of acute pancreatitis that were managed conservatively. He reports no history of such episodes in his relatives and denies a family history of any cardiovascular or gastrointestinal disorders. The vital signs include: blood pressure 105/70 mm Hg, heart rate 101/min, respiratory rate 17/min, and temperature 37.4℃ (99.3℉). The physical examination reveals epigastric tenderness, slight muscle guarding, a positive Mayo-Robson’s sign, and abdominal distention. Laboratory studies show the following findings: Complete blood count Erythrocytes 4.5 x 106/mm3 Hgb 14.7 g/dL Hct 43% Leukocytes 12,700/mm3 Segmented neutrophils 65% Bands 4% Eosinophils 1% Basophils 0% Lymphocytes 27% Monocytes 3% Biochemistry Serum amylase 170 U/L ALT 21 U/L AST 19 U/L Total serum cholesterol 139 mg/dL (3.6 mmol/L) Serum triglycerides 127 mg/dL (1.4 mmol/L) The magnetic resonance cholangiopancreatography findings are shown in the exhibit. What embryogenic disruption could cause such anatomic findings?
A 12-year-old girl with a recently diagnosed seizure disorder is brought to the physician by her mother for genetic counseling. She has difficulties in school due to a learning disability. Medications include carbamazepine. She is at the 95th percentile for height. Genetic analysis shows a 47, XXX karyotype. An error in which of the following stages of cell division is most likely responsible for this genetic abnormality?
A 12-year-old boy follows up with his primary care physician for ongoing management of a urinary tract infection. He recently started middle school and has been having a difficult time navigating the school since he ambulates with leg braces and crutches. Consequently, he has not had sufficient time to use his urinary catheter appropriately. Otherwise, he has been unchanged from the previous visit with both sensory and motor defects in his lower extremities. He has had these defects since birth and has undergone surgeries to repair a bony defect in his spine with protrusion of a membrane through the defect. During what days of embryonic development did the defect responsible for this patient's symptoms most likely occur?
A 34-year-old woman comes to the emergency department because of a 2-hour history of abdominal pain, nausea, and vomiting that began an hour after she finished lunch. Examination shows abdominal guarding and rigidity; bowel sounds are reduced. Magnetic resonance cholangiopancreatography shows the dorsal pancreatic duct draining into the minor papilla and a separate smaller duct draining into the major papilla. The spleen is located anterior to the left kidney. A disruption of which of the following embryological processes is the most likely cause of this patient's imaging findings?
A 69-year-old smoker presents to physician after noticing that his face seems to be more swollen than usual. Upon further questioning, he reports increasing shortness of breath and cough over the past 6 months. On exam, his physician notices venous distention in his neck and distended veins in the upper chest and arms. Chest radiograph shows a right upper lobe mass. What is the embryologic origin of the vessel being compressed by this patient's tumor?
A 21-year-old G3P2 woman presents to her obstetrician at 6 weeks gestation for routine prenatal care. Her past medical history includes obesity and gestational diabetes. She has had two spontaneous vaginal deliveries at term. One infant was macrosomic with hypoglycemia, but otherwise, she has had no complications. Her physician informs her that she must start taking a multivitamin with folic acid daily. The defect that folic acid supplementation protects against arises in tissue that is derived from which germ cell layer?
A child is in the nursery one day after birth. A nurse notices a urine-like discharge being expressed through the umbilical stump. What two structures in the embryo are connected by the structure that failed to obliterate during the embryologic development of this child?
A 35-year-old man comes to the physician for evaluation of a neck mass and hoarseness. He has no history of major medical illness. Physical examination shows a 2.5-cm fixed, irregular thyroid nodule. His serum calcitonin concentration is elevated. The nodule is most likely comprised of cells that are embryologically derived from which of the following structures?
A new imaging modality is being tested to study vitelline duct morphology. A fetus at 20 weeks' gestation is found to have partial obliteration of this duct. Which of the following is the most likely sequela of this condition?
During the third week of development, the blastocyst undergoes a variety of differentiation processes responsible for the formation of the gastrula and, eventually, the embryo. This differentiation creates cell lineages that eventually become a variety of body systems. What cell lineage, present at this date, is responsible for the formation of the liver?
Practice by Chapter
Gametogenesis
Practice Questions
Fertilization and zygote formation
Practice Questions
Cleavage and blastocyst formation
Practice Questions
Implantation
Practice Questions
Bilaminar and trilaminar disc formation
Practice Questions
Neurulation and neural tube development
Practice Questions
Somite formation and derivatives
Practice Questions
Placenta and fetal membranes
Practice Questions
Limb development
Practice Questions
Urogenital system development
Practice Questions
Teratogens and critical periods
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app