
Embryology — MCQs

On this page
What is the pattern of inheritance in neural tube defects?
The covering of an omphalocele is derived from which of the following layers?
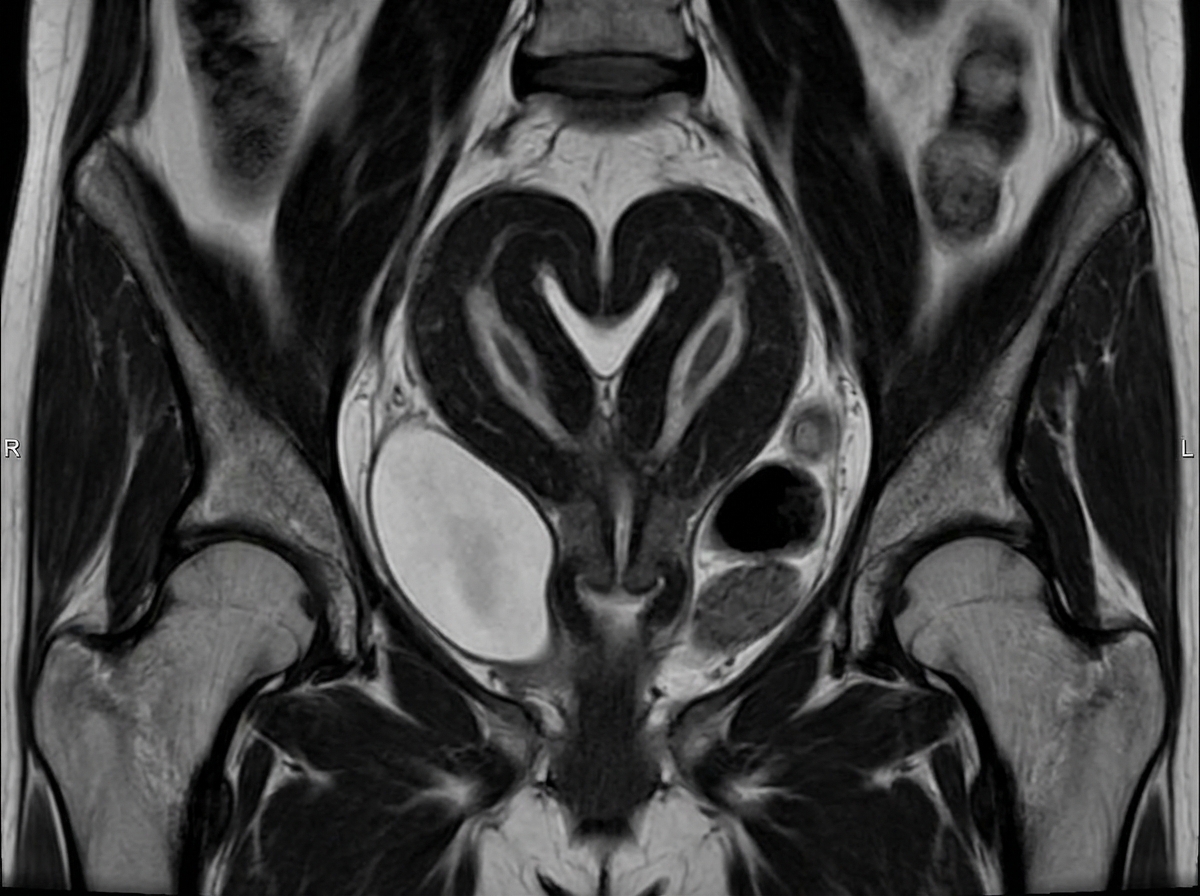
Identify the uterus shown in the image?
Scientists are studying human lung development by trying to identify which proteins and signaling factors trigger lung bud division and bronchiole branching. Their main focus is particularly around the 20th week of gestation, during which terminal bronchioles branch into respiratory bronchioles and further into alveolar ducts. Which of the following phases of embryonic lung development is the stage in which the scientists are interested in studying?
During the obstetric clerkship, the doctor is observing a 3rd-year resident assist a delivery. The patient only had 1 prenatal ultrasound that reported a male fetus. The delivery progresses without complications. The pediatrician-in-charge of the newborn notices a short, broad, upturned penis with an orifice in its dorsal aspect, and both testicles are present in the scrotum. Both the attending and PGY-3 resident immediately recognize the condition. Which of the following female anatomical structures is derived from the embryonic structure affected in this patient?
A primigravid 28-year-old woman delivers a 38-week-old male infant via spontaneous vaginal delivery. She had no prenatal care during her pregnancy. At birth the infant has underdeveloped hands and radiograph reveals missing phalanges in the thumbs. Examination of the buttocks reveals a missing anus. Further work-up reveals flow between the two ventricles on echocardiography and a single kidney on preliminary abdominal ultrasound. The infant also has difficulty feeding that results in coughing and apnea. Which of the following tissues was most likely affected during embryologic development?
A 36-year-old man comes to the physician for a follow-up examination. Two weeks ago, he was diagnosed with an ischemic stroke of the right middle cerebral artery. He was treated with thrombolytics and does not have any residual symptoms. His pulse is 82/min and regular. Cardiovascular examination shows no abnormalities. Echocardiography shows a reproducible, transient, low-volume, right-to-left shunt through the atrial septum during coughing. Which of the following conditions is caused by failure of an embryologic process similar to that responsible for this patient's heart condition?
A newborn boy born vaginally to a healthy 37-year-old G3P1 from a pregnancy complicated by hydramnios fails to pass meconium after 24 hours of life. The vital signs are within normal limits for his age. The abdomen is distended, the anus is patent, and the rectal examination reveals pale mucous with non-pigmented meconium. Based on a barium enema, the boy is diagnosed with sigmoid colonic atresia. Disruption of which structure during fetal development could lead to this anomaly?
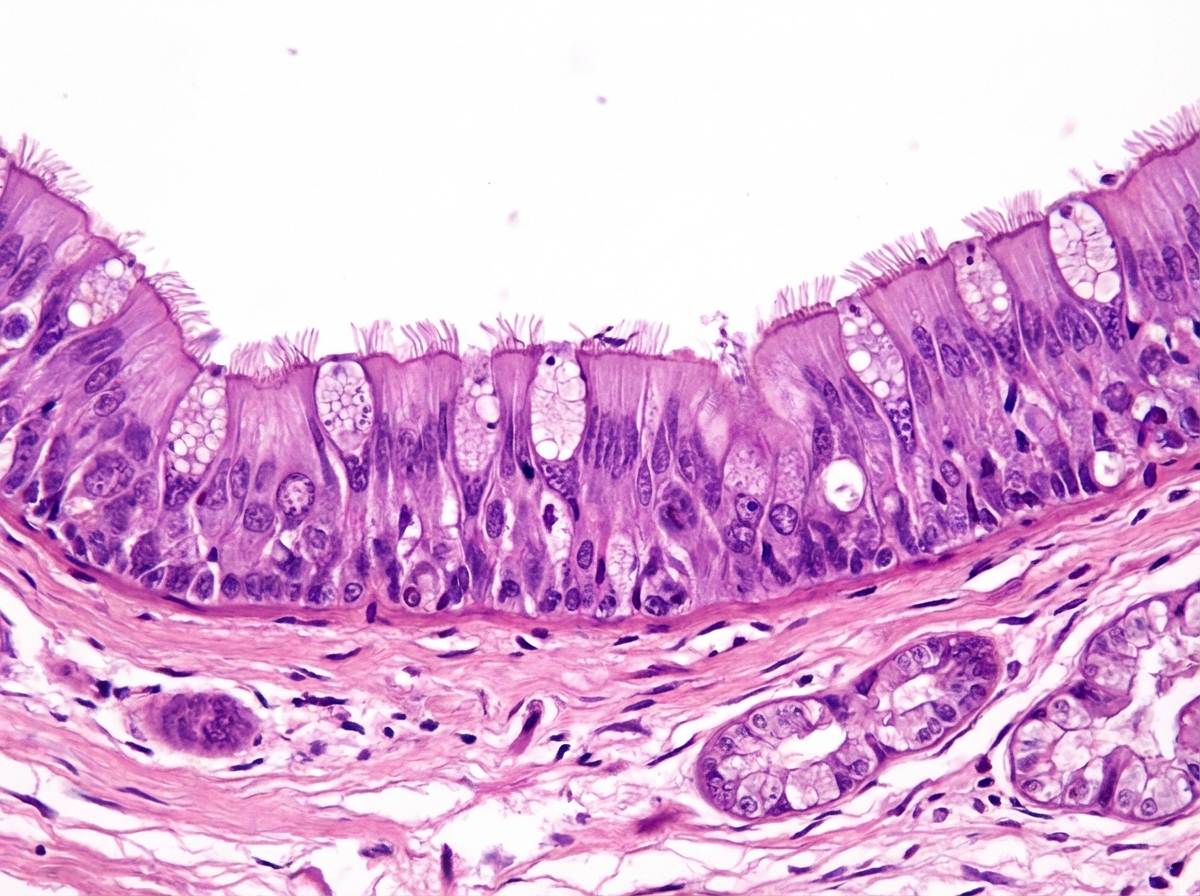
A research team is studying certain congenital anomalies of the respiratory tract. The method consists of marking a certain germinal layer with an isotope, following its development stages in chicken embryos, and finally analyzing the specimen. A given specimen of tissue is presented in the exhibit. Which of the following germinal structures most likely gave rise to the epithelial lining of this specimen?
A 26-year-old woman comes to the physician because she has not had a menstrual period for 5 weeks. Menarche was at the age of 14 years and menses occurred at regular 30-day intervals. She reports having unprotected sexual intercourse 3 weeks ago. A urine pregnancy test is positive. Which of the following best describes the stage of development of the embryo at this time?
Practice by Chapter
Gametogenesis
Practice Questions
Fertilization and zygote formation
Practice Questions
Cleavage and blastocyst formation
Practice Questions
Implantation
Practice Questions
Bilaminar and trilaminar disc formation
Practice Questions
Neurulation and neural tube development
Practice Questions
Somite formation and derivatives
Practice Questions
Placenta and fetal membranes
Practice Questions
Limb development
Practice Questions
Urogenital system development
Practice Questions
Teratogens and critical periods
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app