
Origin and course of anterior corticospinal tract — MCQs

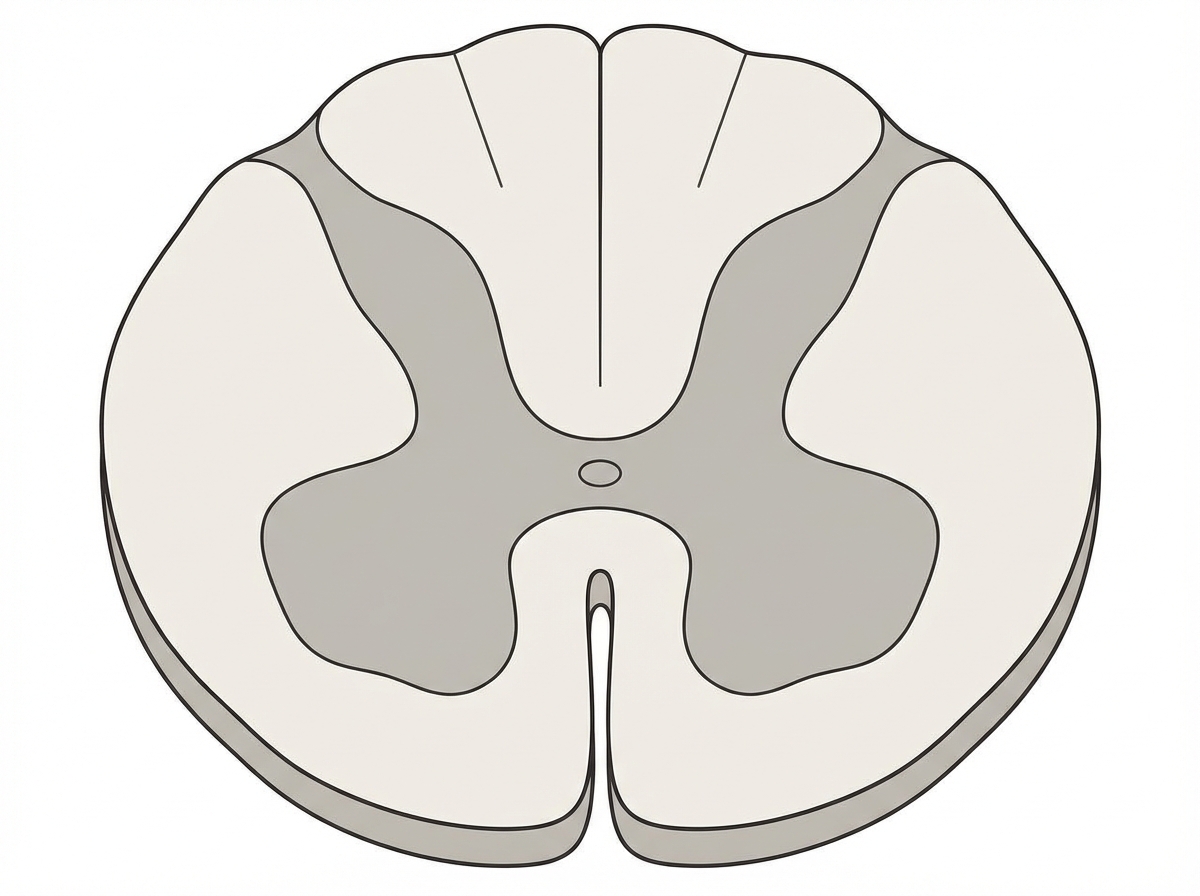
A 45-year-old man is brought to the emergency department by ambulance after a motor vehicle collision. He is not responsive to verbal commands and is unable to provide any history. His pulse is 108/min and regular. Physical examination shows ecchymoses over the neck and back. Neurological examination indicates damage to the spinal cord at the level shown in the illustration. This patient's injury is most likely located at which of the following levels of the spinal cord?
A neurology resident sees a stroke patient on the wards. This 57-year-old man presented to the emergency department after sudden paralysis of his right side. He was started on tissue plasminogen activator within 4 hours, as his wife noticed the symptoms and immediately called 911. When the resident asks the patient how he is doing, he replies by saying that his apartment is on Main St. He does not seem to appropriately answer the questions being asked, but rather speaks off topic. He is able to repeat the word "fan." His consciousness is intact, and his muscle tone and reflexes are normal. Upon striking the lateral part of his sole, his big toe extends upward and the other toes fan out. Which of the following is the area most likely affected in his condition?
A 17-year-old boy is brought to the emergency department after being stabbed with a knife during an altercation. Physical examination shows a 4-cm stab wound on the right lateral border of the T1 spinous process. An MRI of the spinal cord shows damage to the area of the right lateral corticospinal tract at the level of T1. Further evaluation will most likely show which of the following findings?
A 37-year-old man presents to his primary care provider complaining of bilateral arm numbness. He was involved in a motor vehicle accident 3 months ago. His past medical history is notable for obesity and psoriatic arthritis. He takes adalimumab. His temperature is 99.3°F (37.4°C), blood pressure is 130/85 mmHg, pulse is 90/min, and respirations are 18/min. On exam, superficial skin ulcerations are found on his fingers bilaterally. His strength is 5/5 bilaterally in shoulder abduction, arm flexion, arm extension, wrist extension, finger abduction, and thumb flexion. He demonstrates loss of light touch and pinprick response in the distal tips of his 2nd and 5th fingertips and over the first dorsal web space. Vibratory sense is intact in the bilateral upper and lower extremities. Which of the following nervous system structures is most likely affected in this patient?
A 28-year-old male presents to his primary care physician with complaints of intermittent abdominal pain and alternating bouts of constipation and diarrhea. His medical chart is not significant for any past medical problems or prior surgeries. He is not prescribed any current medications. Which of the following questions would be the most useful next question in eliciting further history from this patient?
A 26-year-old woman presents to the obstetrics ward to deliver her baby. The obstetrician establishes a pudendal nerve block via intravaginal injection of lidocaine near the tip of the ischial spine. From which of the following nerve roots does the pudendal nerve originate?
A 61-year-old man is brought to the emergency department by his son after collapsing to the ground while at home. His son immediately performed cardiopulmonary resuscitation and later the patient underwent successful defibrillation after being evaluated by the emergency medical technician. The patient has a medical history of hypertension, hyperlipidemia, and type II diabetes mellitus. He has smoked one-half pack of cigarettes for approximately 30 years. The patient was admitted to the cardiac intensive care unit, and after a few days developed acute onset right upper extremity weakness. His temperature is 99°F (37.2°C), blood pressure is 145/91 mmHg, pulse is 102/min and irregularly irregular, and respirations are 16/min. On physical examination, the patient is alert and orientated to person, place, and time. His language is fluent and he is able to name, repeat, and read. His strength is 5/5 throughout except in the right hand, wrist, and arm, which is 2/5. Based on this patient's clinical presentation, the affected neuronal fibers decussate at which level of the central nervous system?
A 54-year-old man is referred to a tertiary care hospital with a history of 5 months of progressive difficulty in walking and left leg numbness. He first noticed mild gait unsteadiness and later developed gradual right leg weakness. His left leg developed progressive numbness and tingling. His blood pressure is 138/88 mm Hg, the heart rate is 72/min, and the temperature is 36.7°C (98.2°F). On physical examination, he is alert and oriented to person, place, and time. Cranial nerves are intact. Muscle strength is 5/5 in both upper extremities and left lower extremity, but 3/5 in the right leg with increased tone. The plantar reflex is extensor on the right. Pinprick sensation is decreased on the left side below the umbilicus. Vibration and joint position senses are decreased in the right foot and leg. All sensations are normal in the upper extremities. Finger-to-nose and heel-to-shin testing are normal. This patient’s lesion is most likely located in which of the following parts of the nervous system?
A 75-year-old man comes to his primary care physician because he has been having diarrhea and difficulty breathing. The diarrhea has been intermittent with frequent watery stools that occur along with abdominal cramps. Furthermore, the skin on his face and upper chest feels hot and changes color in episodes lasting from a few minutes to hours. Finally, the patient complains of loss of appetite and says that he has unexpectedly lost 20 pounds over the last two months. Based on clinical suspicion, magnetic resonance imaging is obtained showing a small mass in this patient's lungs. Which of the following is associated with the most likely cause of this patient's symptoms?
A 70-year-old man is admitted with fever, chills, and rigor which have lasted for 4 days. He also complains of associated recent-onset fatigue. Past medical history is insignificant. He drinks a can of beer every night. His temperature is 39.0°C (102.2°F), pulse is 120/min, blood pressure is 122/80 mm Hg, and respirations are 14/min. Physical examination reveals splinter hemorrhages in the fingernails, and a 2/6 apical pansystolic murmur is heard which was not present during his last visit a month ago. A transoesophageal echocardiogram shows evidence of vegetations over the mitral valve. Blood cultures are taken from 3 different sites, which reveal the growth of Streptococcus gallolyticus. The patient is started on the appropriate antibiotic therapy which results in rapid clinical improvement. Which of the following would be the best next step in management in this patient after he is discharged?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app