
Brainstem nuclei — MCQs

On this page
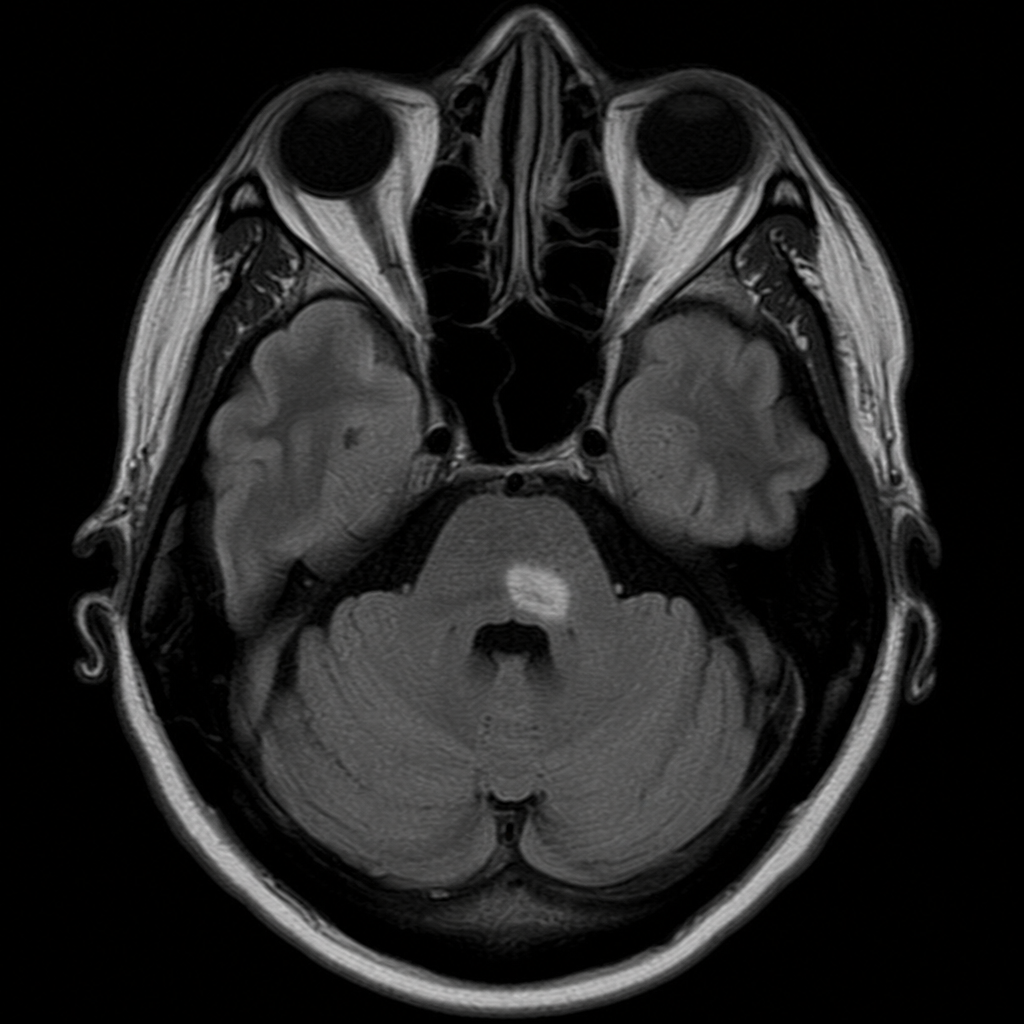
A 67-year-old man with a history of atrial fibrillation presents with sudden onset of right-sided facial droop involving the forehead, inability to conjugately gaze to the right, and left-sided hemiplegia sparing the face. His pupils are equal and reactive. An MRI is obtained. At which axial level and side does the lesion most likely reside?
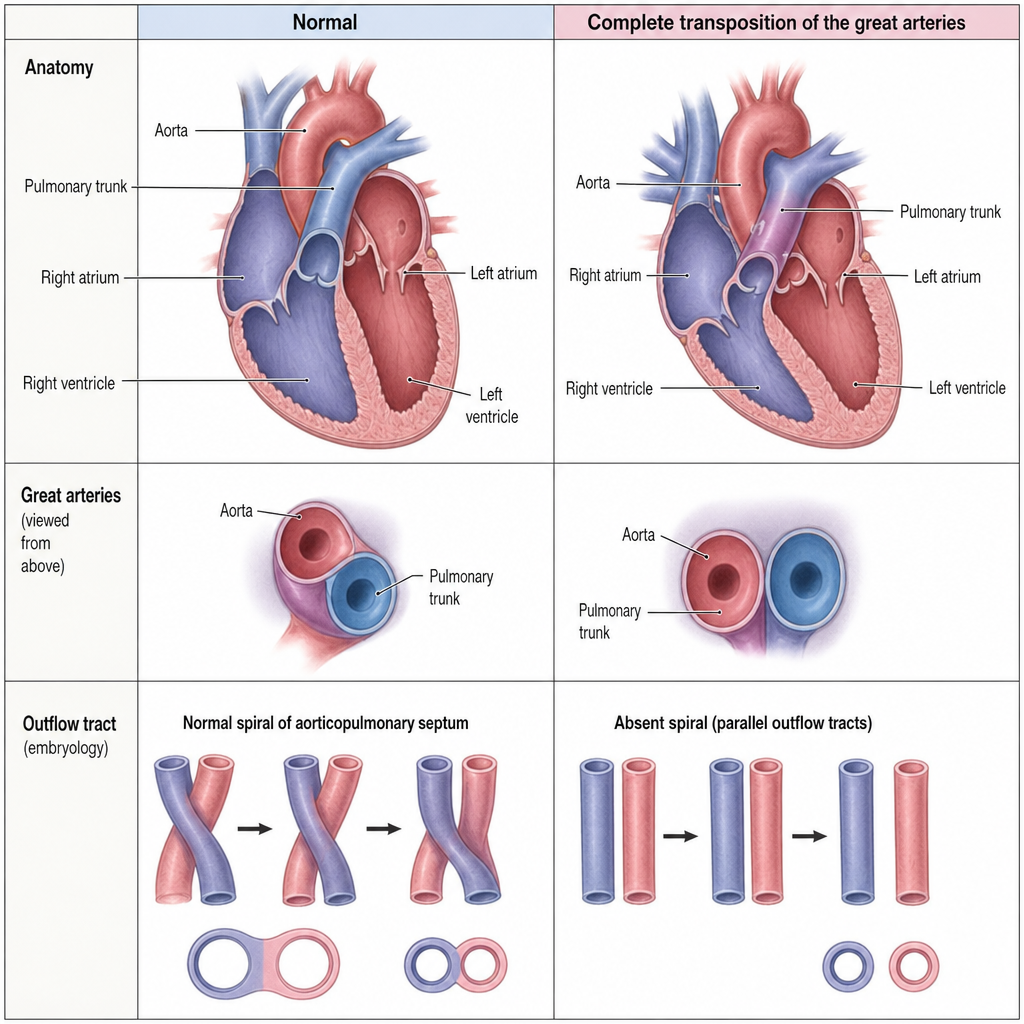
A 32-year-old woman at 28 weeks of gestation undergoes a fetal echocardiogram that reveals the aorta arising from the morphological right ventricle and the pulmonary trunk arising from the morphological left ventricle. The great vessels run parallel rather than in their normal spiral relationship. The embryological error most directly responsible for this anomaly occurred during which developmental process?
An 86-year-old woman is brought to the emergency department by her niece because the patient felt like she was spinning and about to topple over. This occurred around 4 hours ago, and although symptoms have improved, she still feels like she is being pulled to the right side. The vital signs include: blood pressure 116/75 mm Hg, pulse 90/min, and SpO2 99% on room air. Physical examination reveals right-sided limb ataxia along with hypoalgesia and decreased temperature sensation on the right side of the face and left side of the body. An urgent non-contrast CT scan of the head shows no evidence of hemorrhage. What other finding is most likely to be present in this patient?
A 60-year-old woman presents with progressive difficulty swallowing solid foods for the past 2 months. She also says her voice has gradually changed, and she has had recent episodes of vertigo associated with nausea and vomiting and oscillating eye movements while reading. She denies any problems with the movement of her face or extremities. Past medical history is significant for hypertension, managed with enalapril, and dyslipidemia, which she is managing with dietary modifications. The patient reports a 40-pack-year smoking history. Vital signs are within normal limits. On physical examination, there is decreased pain and temperature sensation on the right side of her body, and she cannot touch her nose with her eyes closed. Which of the following is the most likely site of vascular occlusion in this patient?
A 59-year-old woman with a past medical history of atrial fibrillation currently on warfarin presents to the emergency department for acute onset dizziness. She was watching TV in the living room when she suddenly felt the room spin around her as she was getting up to go to the bathroom. She denies any fever, weight loss, chest pain, palpitations, shortness of breath, lightheadedness, or pain but reports difficulty walking and hiccups. A physical examination is significant for rotary nystagmus and decreased pin prick sensation on the left side of her body. A magnetic resonance image (MRI) of the head is obtained and shows ischemic changes of the right lateral medulla. What other symptoms would you expect to find in this patient?
A 65-year-old man is brought into the emergency department by his wife for slurred speech and right-sided weakness. The patient has a significant past medical history of hypertension and hyperlipidemia. The wife reports her husband went to bed last night normally but woke up this morning with the symptoms mentioned. Physical examination shows right-sided hemiparesis along with the loss of vibration and proprioception. Cranial nerve examination shows a deviated tongue to the left. What is the most likely diagnosis?
A 56-year-old man with a significant past medical history of diabetes mellitus, hypertension, and hypercholesterolemia is brought to the emergency department by his wife. The wife states the symptoms started 1 hour ago when she noticed that he was having difficulty swallowing his breakfast and that his voice was hoarse. The patient had a recent admission for a transient ischemic attack but was not compliant with his discharge instructions and medication. Examination of the eye shows left-sided partial ptosis and miosis along with diplopia and nystagmus. During the examination, it is noted that the right side of the face and body has markedly more sweating than the left side. An MRI of the brain reveals an ischemic infarct at the level of the left lateral medulla. Which of the following most likely accounts for this patient’s symptoms?
A 73-year-old woman is brought in by her daughter stating that her mom has become increasingly forgetful and has trouble remembering recent events. Her memory for remote events is remarkably intact. The patient is no longer able to cook for herself as she frequently leaves the stove on unattended. She has recently been getting lost in her neighborhood even though she has lived there for 30 years. Her mood is not depressed. Decreased activity in which of the following areas of the brain is known to be involved in the pathogenesis of Alzheimer's disease?
A 72-year-old woman is brought in to the emergency department after her husband noticed that she appeared to be choking on her dinner. He performed a Heimlich maneuver but was concerned that she may have aspirated something. The patient reports a lack of pain and temperature on the right half of her face, as well as the same lack of sensation on the left side of her body. She also states that she has been feeling "unsteady" on her feet. On physical exam you note a slight ptosis on the right side. She is sent for an emergent head CT. Where is the most likely location of the neurological lesion?
A 55-year-old man is brought to the emergency department by his wife after falling down. About 90 minutes ago, they were standing in their kitchen making lunch and chatting when he suddenly complained that he could not see as well, felt weak, and was getting dizzy. He began to lean to 1 side, and he eventually fell to the ground. He did not hit his head. In the emergency department, he is swaying while seated, generally leaning to the right. The general physical exam is unremarkable. The neurologic exam is notable for horizontal nystagmus, 3/5 strength in the right arm, ataxia of the right arm, and absent pinprick sensation in the left arm and left leg. The computed tomography (CT) scan of the head is unremarkable. Which of the following is the most likely single location of this patient's central nervous system lesion?
Practice by Chapter
Medulla oblongata nuclei
Practice Questions
Pontine nuclei
Practice Questions
Midbrain nuclei
Practice Questions
Cranial nerve nuclei
Practice Questions
Reticular formation
Practice Questions
Ascending sensory pathways in brainstem
Practice Questions
Descending motor pathways in brainstem
Practice Questions
Vestibular nuclei complex
Practice Questions
Vital centers in brainstem
Practice Questions
Brainstem lesions and clinical correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app