
Vascular Surgery — MCQs

On this page
In a patient with chronic thromboembolic pulmonary hypertension, what is the rationale for choosing pulmonary thromboendarterectomy (PTE) over medical management?
In a patient with carotid artery stenosis, how should the decision for carotid endarterectomy be determined?
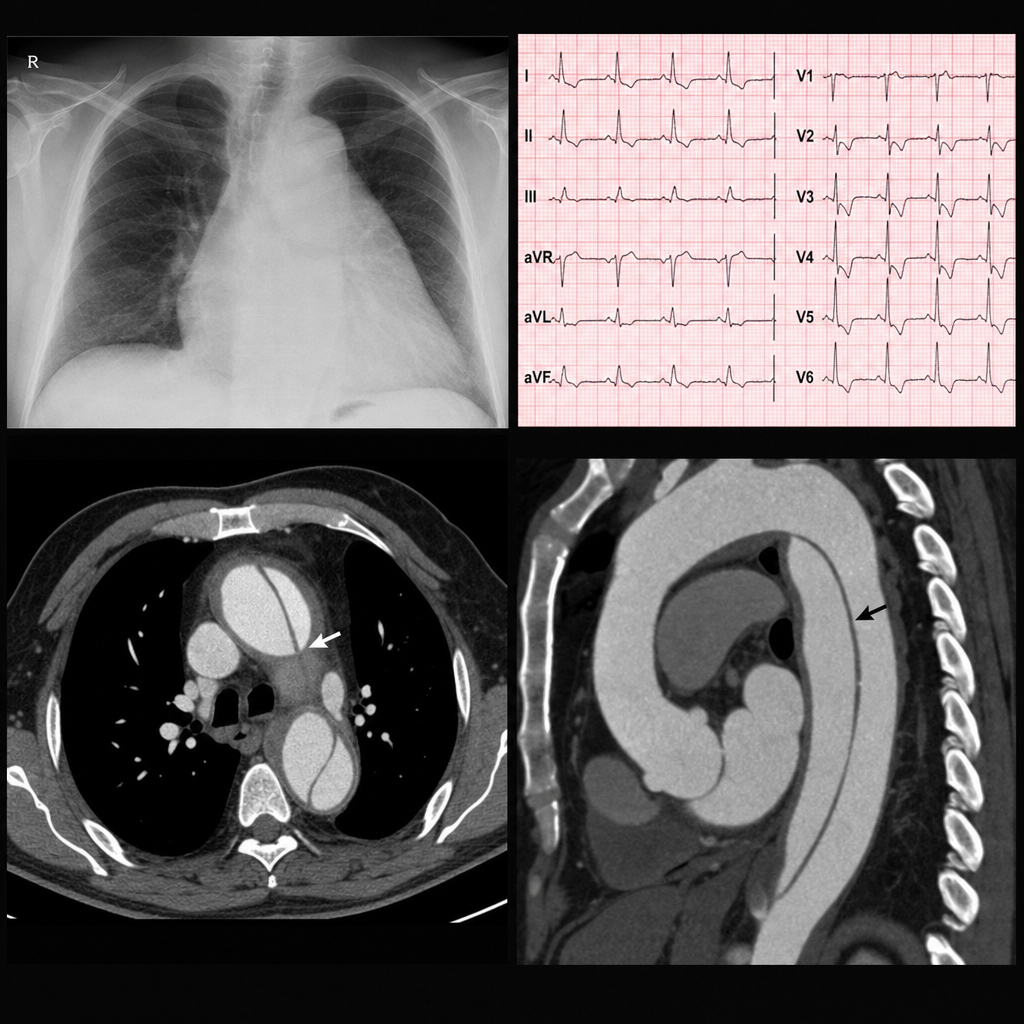
A 62-year-old man with a history of hypertension and diabetes presents with chest pain radiating to the back, a blood pressure of 220/110 mmHg, ST depression in leads V4-V6 on ECG, and a chest X-ray showing a wide mediastinum. He then develops left-sided weakness and slurred speech, with his blood pressure dropping to 90/60 mmHg. What is the diagnosis and the next step in management?
A 70-year-old man presents with severe pain in his right lower limb. Upon examination, the limb is cold, pale, and pulseless. What is the most likely diagnosis?
Which complication is most commonly associated with untreated varicose veins?
In a patient with acute limb ischemia and evidence of thrombotic occlusion, what is the treatment of choice?
A 65-year-old male, diabetic and a smoker, presents with a non-healing ulcer and absent pulses in the right foot, with a TcPO2 of 20 mmHg. The left foot shows claudication and an ABI of 0.6. An angiogram reveals right SFA occlusion and left SFA 70% stenosis. What is the best surgical approach?
A 68-year-old male with type 2 diabetes mellitus presents with severe lower extremity pain, pallor, and pulselessness. Examination reveals a cool extremity and absent femoral pulses, with an ankle-brachial index (ABI) of less than 0.5. Evaluate and select the optimal treatment approach.
A 60-year-old male with a history of smoking presents with severe abdominal pain and a pulsatile abdominal mass. What is the most appropriate next step in managing this patient?
Which treatment is considered more effective for the management of varicose veins in terms of long-term outcomes and recurrence rates?
Practice by Chapter
Atherosclerotic Disease
Practice Questions
Aortic Aneurysms
Practice Questions
Peripheral Arterial Disease
Practice Questions
Carotid Artery Disease
Practice Questions
Venous Thromboembolism
Practice Questions
Chronic Venous Insufficiency
Practice Questions
Mesenteric Vascular Disease
Practice Questions
Vascular Trauma
Practice Questions
Vascular Access for Hemodialysis
Practice Questions
Endovascular Techniques
Practice Questions
Diabetic Foot Vascular Disease
Practice Questions
Vasculitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app