
Vascular Surgery — MCQs

On this page
A 68-year-old male smoker presents with rest pain in his right foot, absent dorsalis pedis and posterior tibial pulses, cool and pale skin distally, and an ankle-brachial index of 0.4. What type of ulcer is shown below?

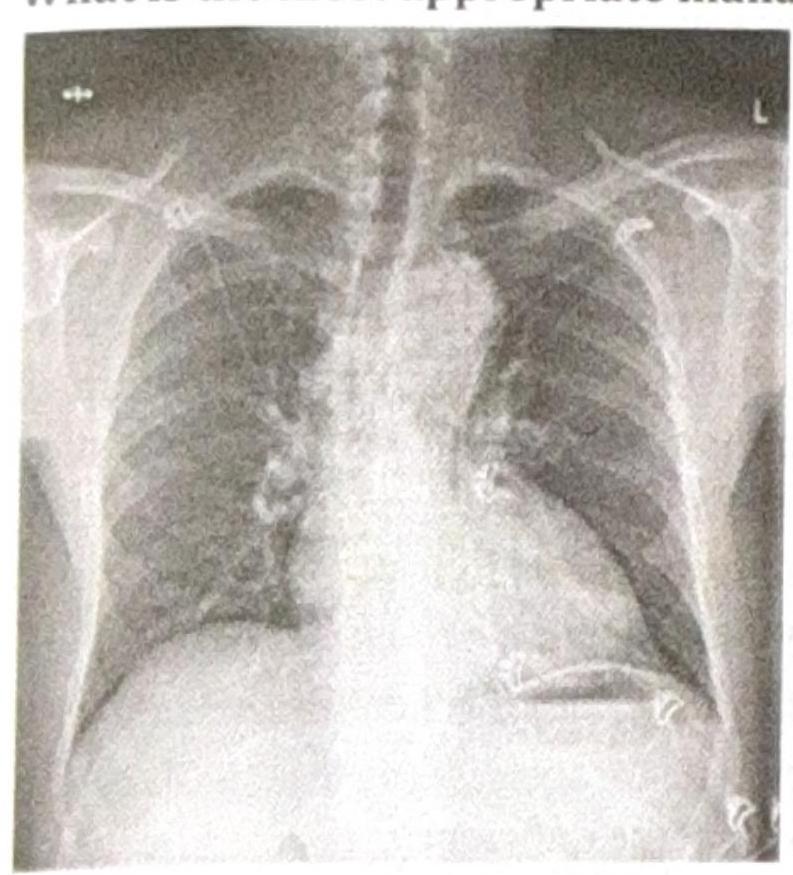
A patient presents with constant chest pain. The chest radiograph shows a widened mediastinum, and CT angiography confirms an acute Stanford Type A aortic dissection involving the ascending aorta. What is the most appropriate definitive management?
A hypertensive patient presents with excruciating chest pain and unequal radial pulses. Which of the following is the correct management for this patient?
Asymptomatic varicose veins would fall under which category of the CEAP classification system?
A patient presents with dull aching pain and tortuous veins in both lower limbs. Which test would be appropriate for evaluating saphenofemoral junction (SFJ) incompetence?
During a surgical procedure to repair an abdominal aortic aneurysm, the surgeon must be careful to avoid injury to which of the following arterial structures that originates near the level of the renal vessels?
A 72-year-old man presents to his primary care physician because he has been having flank and back pain for the last 8 months. He said that it started after he fell off a chair while doing yard work, but it has been getting progressively worse over time. He reports no other symptoms and denies any weight loss or tingling in his extremities. His medical history is significant for poorly controlled hypertension and a back surgery 10 years ago. He drinks socially and has smoked 1 pack per day since he was 20. His family history is significant for cancer, and he says that he is concerned that his father had similar symptoms before he was diagnosed with multiple myeloma. Physical exam reveals a painful, pulsatile enlargement in the patient's abdomen. Between which of the following locations has the highest risk of developing this patient's disorder?
A 71-year-old man comes to the physician for a routine health maintenance examination. He feels well. He goes for a 30-minute walk three times a week and does not experience any shortness of breath or chest or leg pain on exertion. He has not had any weakness, numbness, or vision disturbance. He has diabetes that is well controlled with insulin injections. He had smoked one pack of cigarettes every day for 40 years but quit 5 years ago. He appears healthy and well nourished. His temperature is 36.3°C (97.3°F), pulse is 75/min, and blood pressure is 136/78 mm Hg. Physical examination shows normal heart sounds. There are systolic bruits over the neck bilaterally. Physical and neurologic examinations show no other abnormalities. Fasting serum studies show: Total cholesterol 210 mg/dL HDL cholesterol 28 mg/dL LDL cholesterol 154 mg/dL Triglycerides 140 mg/dL Glucose 102 mg/dL Duplex ultrasonography of the carotid arteries shows a 85% stenosis on the left and a 55% stenosis on the right side. Which of the following is the most appropriate next step in management?
A 45-year-old policeman presents with pain in the right leg after duty. On examination, the pulse in the right popliteal fossa is absent, and there is pain in the right buttock. The left side is normal. At which level is the blockage?
A patient with varicose veins came to the hospital; an intern was on duty. Which test should he perform to assess the competency of deep veins?
Practice by Chapter
Atherosclerotic Disease
Practice Questions
Aortic Aneurysms
Practice Questions
Peripheral Arterial Disease
Practice Questions
Carotid Artery Disease
Practice Questions
Venous Thromboembolism
Practice Questions
Chronic Venous Insufficiency
Practice Questions
Mesenteric Vascular Disease
Practice Questions
Vascular Trauma
Practice Questions
Vascular Access for Hemodialysis
Practice Questions
Endovascular Techniques
Practice Questions
Diabetic Foot Vascular Disease
Practice Questions
Vasculitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app