
Vascular Surgery — MCQs

On this page
A male patient presented with a sudden onset tearing type of chest pain radiating to the back, shortness of breath, and nausea. CT chest image is given. What is the most appropriate next step in the management of this patient?
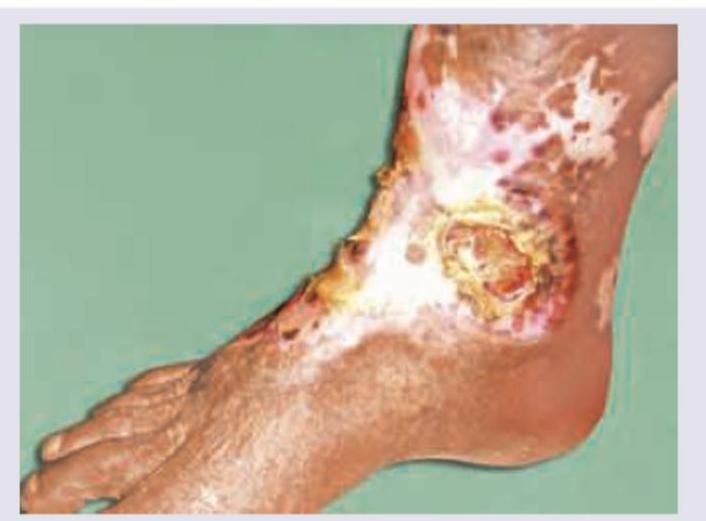
A 73 year old male smoker with a past history of coronary artery disease presents with blackening of the toes. An image of the foot is shown below. What is the most likely diagnosis?
A 60-year-old male presents with claudication and blackening of the toes. An image of the foot is shown below. What is the most likely diagnosis? 
Imminent gangrene is seen at which Ankle-Brachial Pressure Index (ABPI)?
A 56-year-old man presents with the following pathology shown in the image, which of the following is correct?
History of pulsatile mass in the neck. Digital angiography image shown. Not filling on carotid compression. But refilling on releasing pressure. What is the diagnosis?
What is the most probable diagnosis of a patient whose clinical presentation is shown below?
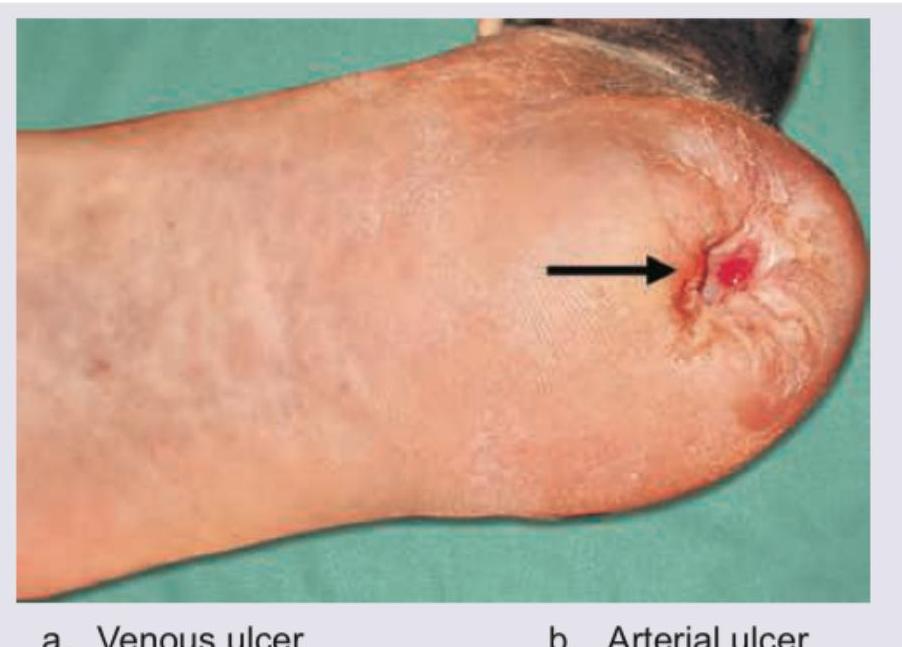
A patient presents with a heel ulcer. Examination reveals absent pedal pulses, cool skin, rest pain that is relieved with dependency, and an ankle-brachial index of 0.4. Identify the type of ulcer shown on the heel of the foot.
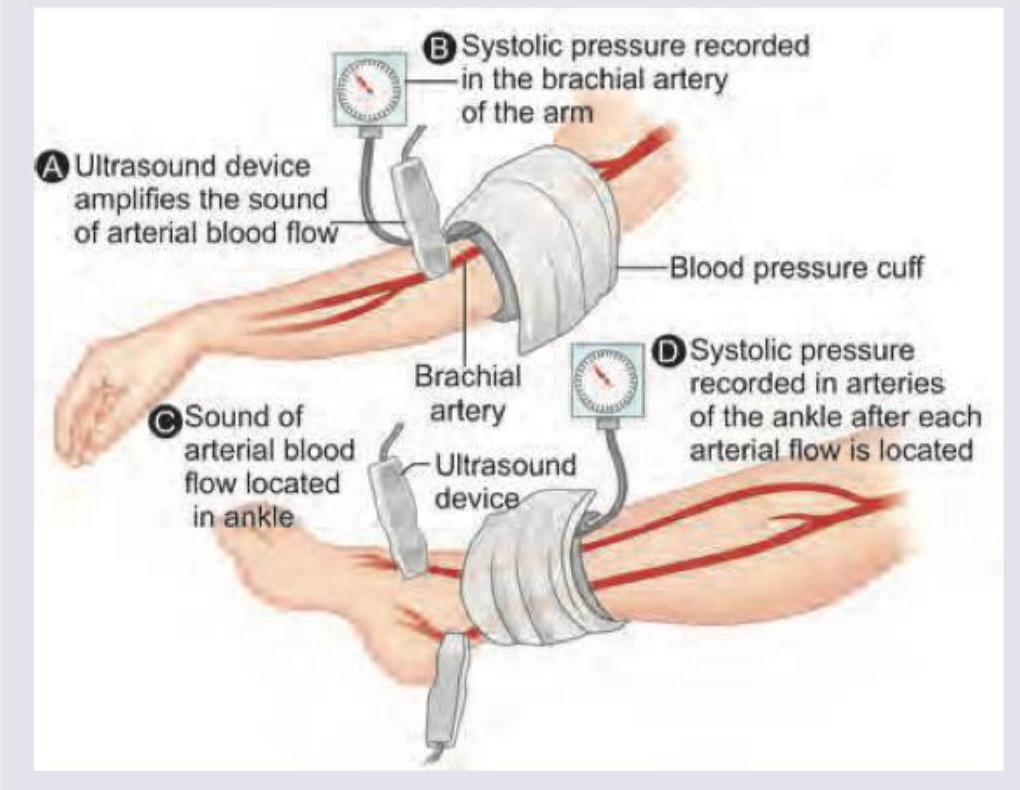
The following test was performed on a patient with leg pain on exertion. Which feature best characterizes intermittent claudication?
Which one of the following is correct regarding splenic artery aneurysm?
Practice by Chapter
Atherosclerotic Disease
Practice Questions
Aortic Aneurysms
Practice Questions
Peripheral Arterial Disease
Practice Questions
Carotid Artery Disease
Practice Questions
Venous Thromboembolism
Practice Questions
Chronic Venous Insufficiency
Practice Questions
Mesenteric Vascular Disease
Practice Questions
Vascular Trauma
Practice Questions
Vascular Access for Hemodialysis
Practice Questions
Endovascular Techniques
Practice Questions
Diabetic Foot Vascular Disease
Practice Questions
Vasculitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app