
Vascular Surgery — MCQs

On this page
What is true about carotid body tumors?
Acute vascular ischemia manifests as?
Pseudoaneurysm in a drug abuser is typically seen in which artery?
Passive forcible dorsiflexion of the foot with the knee extended causes pain in the calf. What is this sign called?
Intermittent claudication is seen when the ankle-brachial index is?
Complications arising out of A-V fistula done for renal failure include the following EXCEPT?
A 45-year-old woman presents with right lower extremity swelling and multiple varicosities two months after undergoing cardiac catheterization via a right femoral approach. Examination reveals a bruit over the right groin. What is the most likely diagnosis?
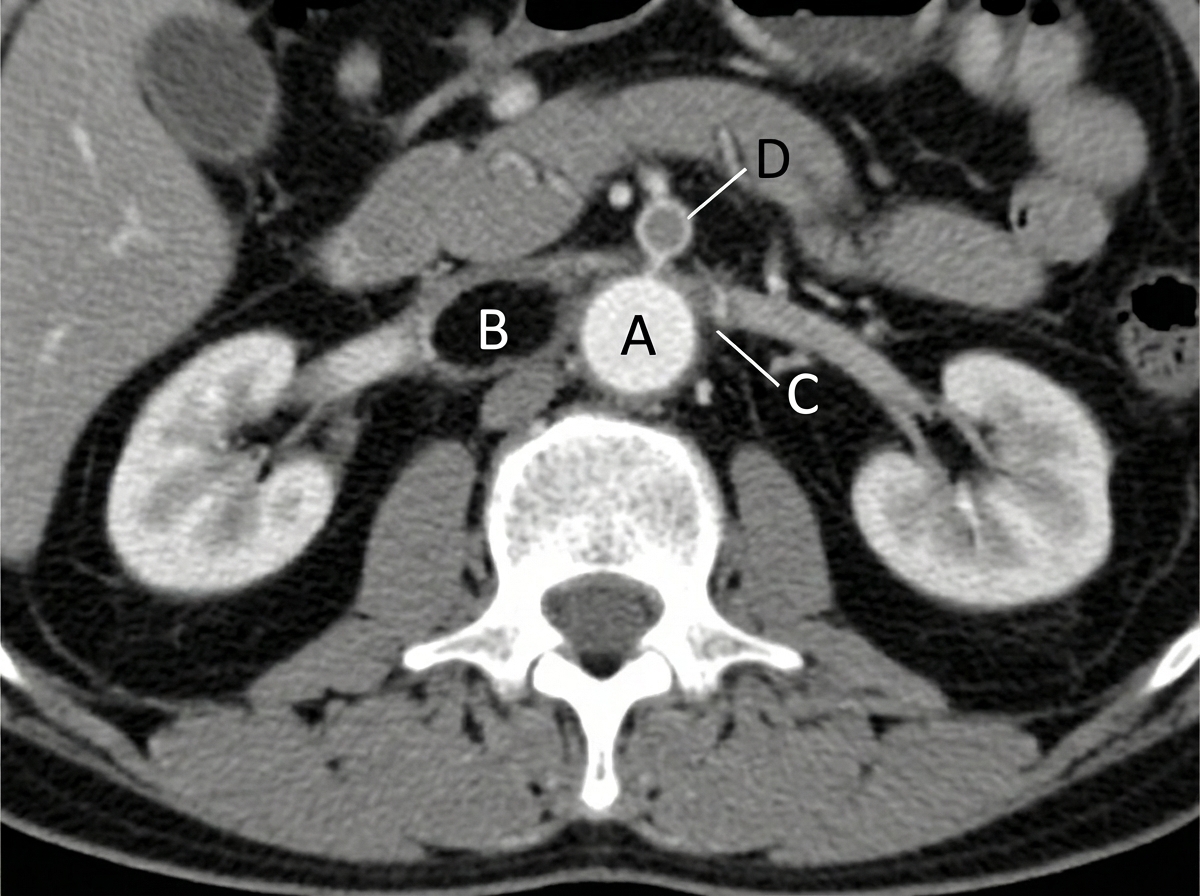
A 70-year-old woman with a history of myocardial ischemia and peripheral vascular disease presented with sudden onset of severe, rapidly increasing epigastric pain, nausea, vomiting, and minimal abdominal tenderness. She was writhing in pain, had normal bowel sounds, and a small amount of blood in her stool. Electrolyte analysis revealed a bicarbonate level of 15 mEq/L, and serum lactate was elevated, indicating tissue hypoxia and injury. A CT scan was planned. What anatomical structure is likely involved?
Which of the following describes stage 3 limb ischemia as per the Fontaine classification?
A 56-year-old man has suffered from intermittent claudication for 5 years. He has recently developed cramping abdominal pain that is made worse by eating. He has a history of a 15-lb weight loss. What is the most likely diagnosis?
Practice by Chapter
Atherosclerotic Disease
Practice Questions
Aortic Aneurysms
Practice Questions
Peripheral Arterial Disease
Practice Questions
Carotid Artery Disease
Practice Questions
Venous Thromboembolism
Practice Questions
Chronic Venous Insufficiency
Practice Questions
Mesenteric Vascular Disease
Practice Questions
Vascular Trauma
Practice Questions
Vascular Access for Hemodialysis
Practice Questions
Endovascular Techniques
Practice Questions
Diabetic Foot Vascular Disease
Practice Questions
Vasculitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app