
Vascular Surgery — MCQs

On this page
The following are true regarding intermittent claudication, except:
What is the most common site for venous thrombosis?
Visceral aneurysm is most commonly seen in which of the following locations?
Which test is NOT used to demonstrate the presence of collateral circulation of the hand?
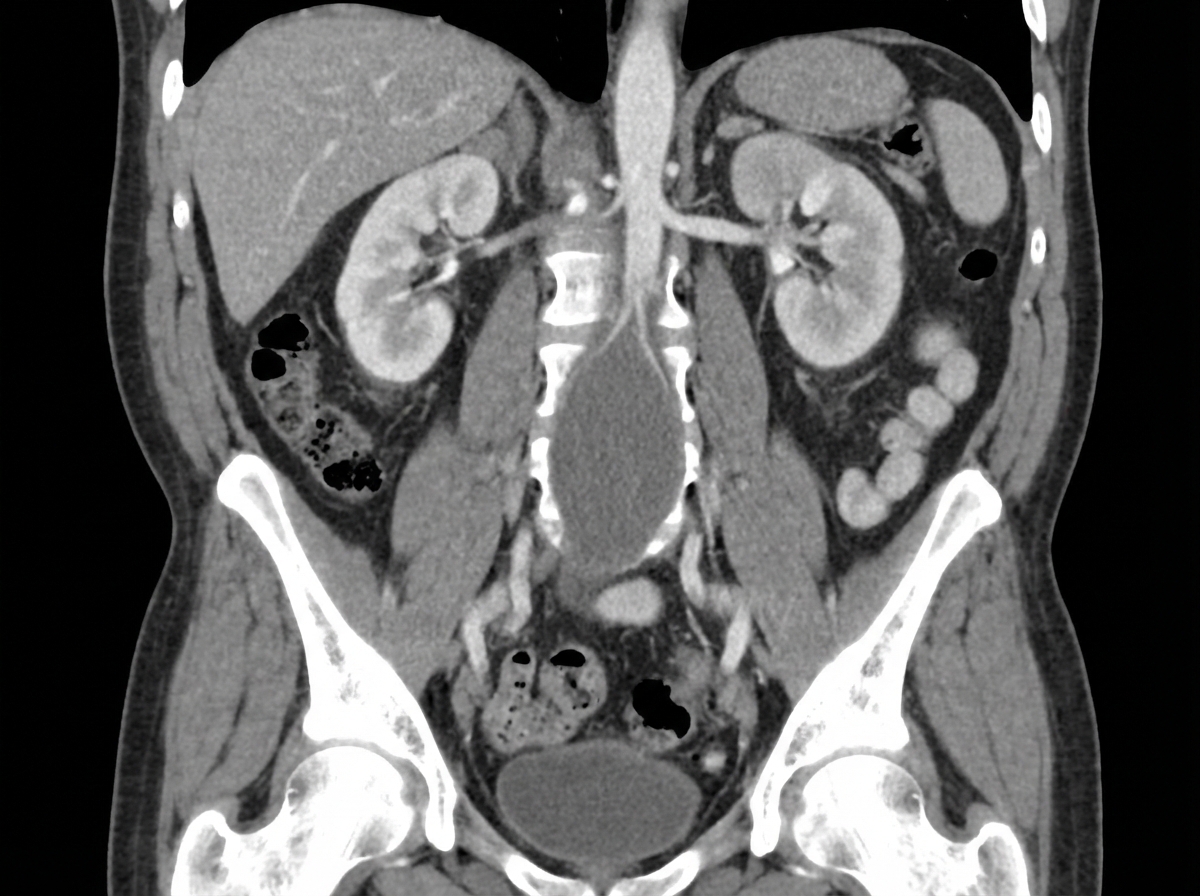
A 70-year-old man presents with right flank pain that radiates to his groin. He has a long history of heavy smoking and alcohol use and reports passing a kidney stone approximately 20 years prior to this event. His past medical history is also remarkable for diabetes mellitus, high cholesterol, and obesity. A computed tomography scan reveals a right 7-mm ureteral stone. In addition, coronal imaging was obtained. Which of the following is the greatest risk factor for the development of additional findings on the imaging study?
Which of the following is NOT true regarding Milroy's disease?
Which of the following are features of Klippel-Trenaunay syndrome?
What is the most common bacterial infection associated with lymphedema?
A 45-year-old male with a history of chronic smoking presents with pain in his lower limb due to blockage of the femoral artery. What is the most likely diagnosis?
Which of the following drugs is NOT used for sclerotherapy of varicose veins?
Practice by Chapter
Atherosclerotic Disease
Practice Questions
Aortic Aneurysms
Practice Questions
Peripheral Arterial Disease
Practice Questions
Carotid Artery Disease
Practice Questions
Venous Thromboembolism
Practice Questions
Chronic Venous Insufficiency
Practice Questions
Mesenteric Vascular Disease
Practice Questions
Vascular Trauma
Practice Questions
Vascular Access for Hemodialysis
Practice Questions
Endovascular Techniques
Practice Questions
Diabetic Foot Vascular Disease
Practice Questions
Vasculitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app