
Vascular Surgery — MCQs

On this page
Diagnosis of thoracic outlet syndrome is made by which one of the following?
What is the most common complication of below-knee stripping of varicose veins?
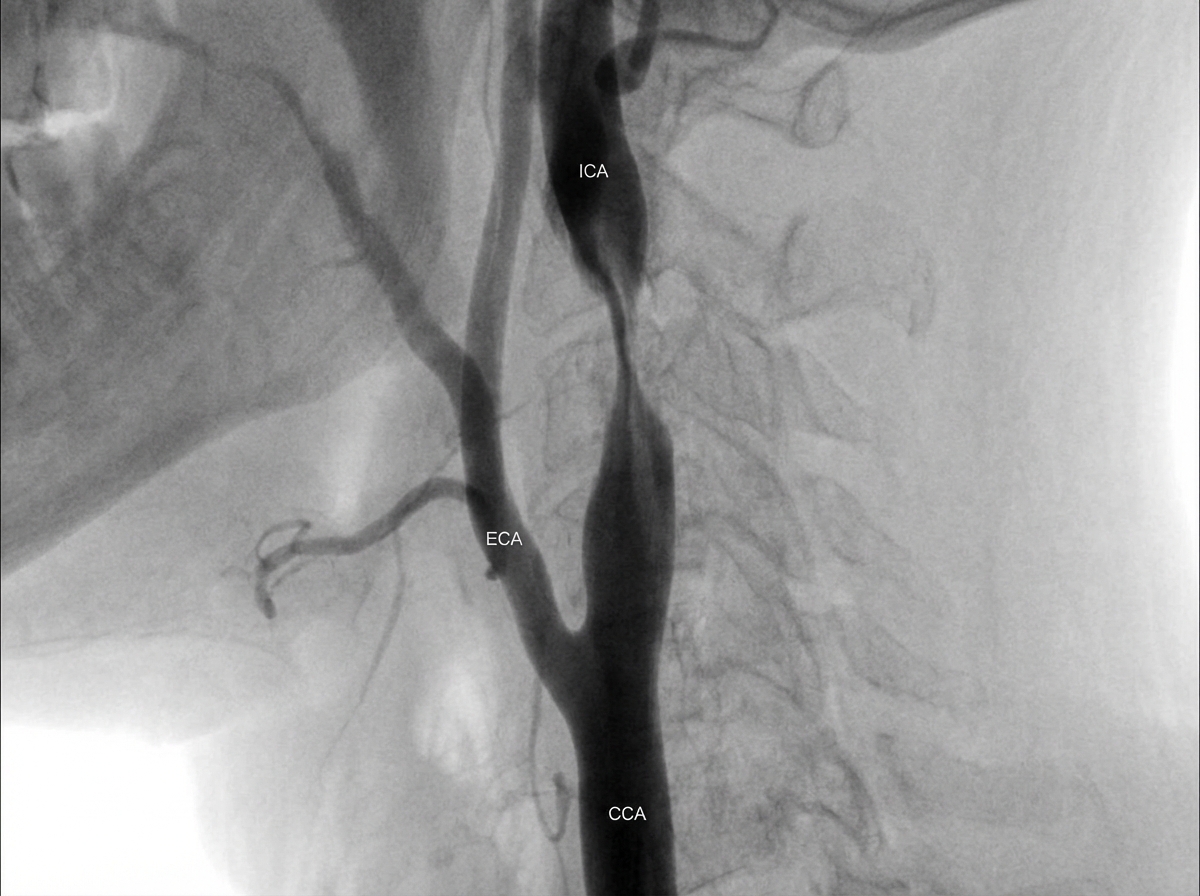
An arteriogram of a 75-year-old man with an asymptomatic carotid bruit, mild hypertension, and mild COPD is shown. The imaging demonstrates asymptomatic internal carotid stenosis of at least 70%, his life expectancy exceeds five years, and the center's anticipated perioperative stroke/death rate is below 3%. Which revascularization strategy may be added to intensive medical therapy in this carefully selected low-operative-risk patient?
A 40-year-old male, a chronic smoker, presents with claudication and a medial leg ulcer. For the past one month, he is experiencing rest pain. Which of the following procedures would not relieve his rest pain?
Which of the following is NOT a risk factor for the development of critical limb ischemia?
Intermittent claudication at the hip level indicates which of the following?
What are the causes of unilateral lymphedema of the leg that should be investigated?
Regarding varicose veins, which one of the following statements is true?
Which of the following statements about carotid stenosis is true?
Which of the following is NOT a bypass procedure used in the surgical management of lymphedema?
Practice by Chapter
Atherosclerotic Disease
Practice Questions
Aortic Aneurysms
Practice Questions
Peripheral Arterial Disease
Practice Questions
Carotid Artery Disease
Practice Questions
Venous Thromboembolism
Practice Questions
Chronic Venous Insufficiency
Practice Questions
Mesenteric Vascular Disease
Practice Questions
Vascular Trauma
Practice Questions
Vascular Access for Hemodialysis
Practice Questions
Endovascular Techniques
Practice Questions
Diabetic Foot Vascular Disease
Practice Questions
Vasculitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app