
Vascular Surgery — MCQs

On this page
Which of the following is true regarding arteriovenous fistula?
Thoracic outlet syndrome is most commonly seen in which age group?
A 67-year-old man presents with sudden left leg pain, absence of pulses, and a cold limb. His past medical history is significant for coronary artery disease and a small aortic aneurysm. Which of the following is most likely responsible for the development of a cold limb in this patient?
Regarding abdominal aortic aneurysm, all are true except?
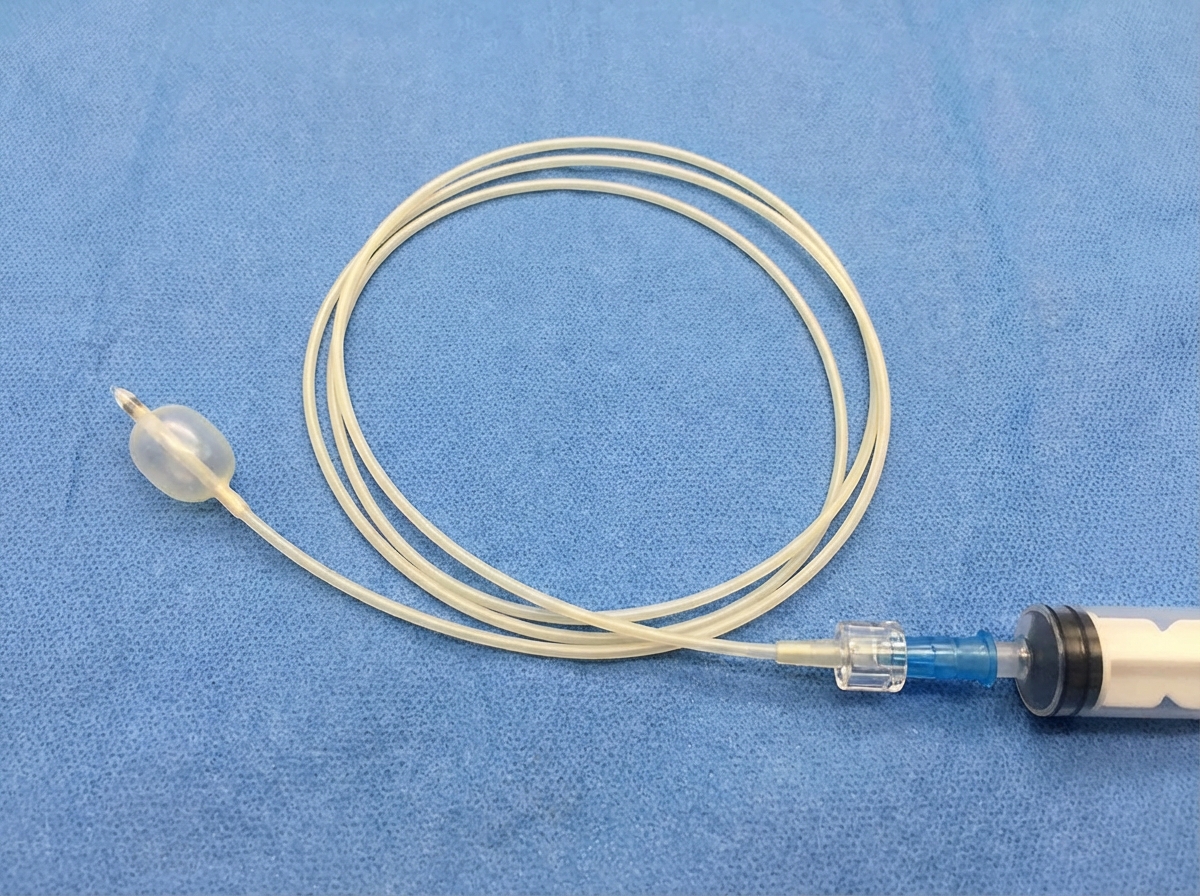
Which instrument is shown in the image?
A 65-year-old female presents for a routine examination and is found to have a pulsatile abdominal mass. She has a history of hypertension but is otherwise healthy. Her father died from a ruptured abdominal aortic aneurysm. What are the acceptable reasons to operate on a 5-cm infrarenal abdominal aortic aneurysm in this patient?
Which statement is NOT true regarding carotid body tumors?
What is true about mesenteric vein thrombosis?
Which of the following is a cause of peripheral arterial occlusive disease?
Which of the following is NOT used in the treatment of superficial venous thrombosis?
Practice by Chapter
Atherosclerotic Disease
Practice Questions
Aortic Aneurysms
Practice Questions
Peripheral Arterial Disease
Practice Questions
Carotid Artery Disease
Practice Questions
Venous Thromboembolism
Practice Questions
Chronic Venous Insufficiency
Practice Questions
Mesenteric Vascular Disease
Practice Questions
Vascular Trauma
Practice Questions
Vascular Access for Hemodialysis
Practice Questions
Endovascular Techniques
Practice Questions
Diabetic Foot Vascular Disease
Practice Questions
Vasculitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app