
Renal Cell Carcinoma — MCQs

The cytogenetics of chromophilic renal cell carcinoma is characterized by:
Management of RCC less than 4 cm in size:
A patient has a cerebellar mass, renal tumor, and a family history of similar conditions. Which of the following mutations is most likely present in the family?
Most common type of renal carcinoma is:
What is the best investigation for diagnosis and staging of renal cell carcinoma with thrombus extending into the IVC?
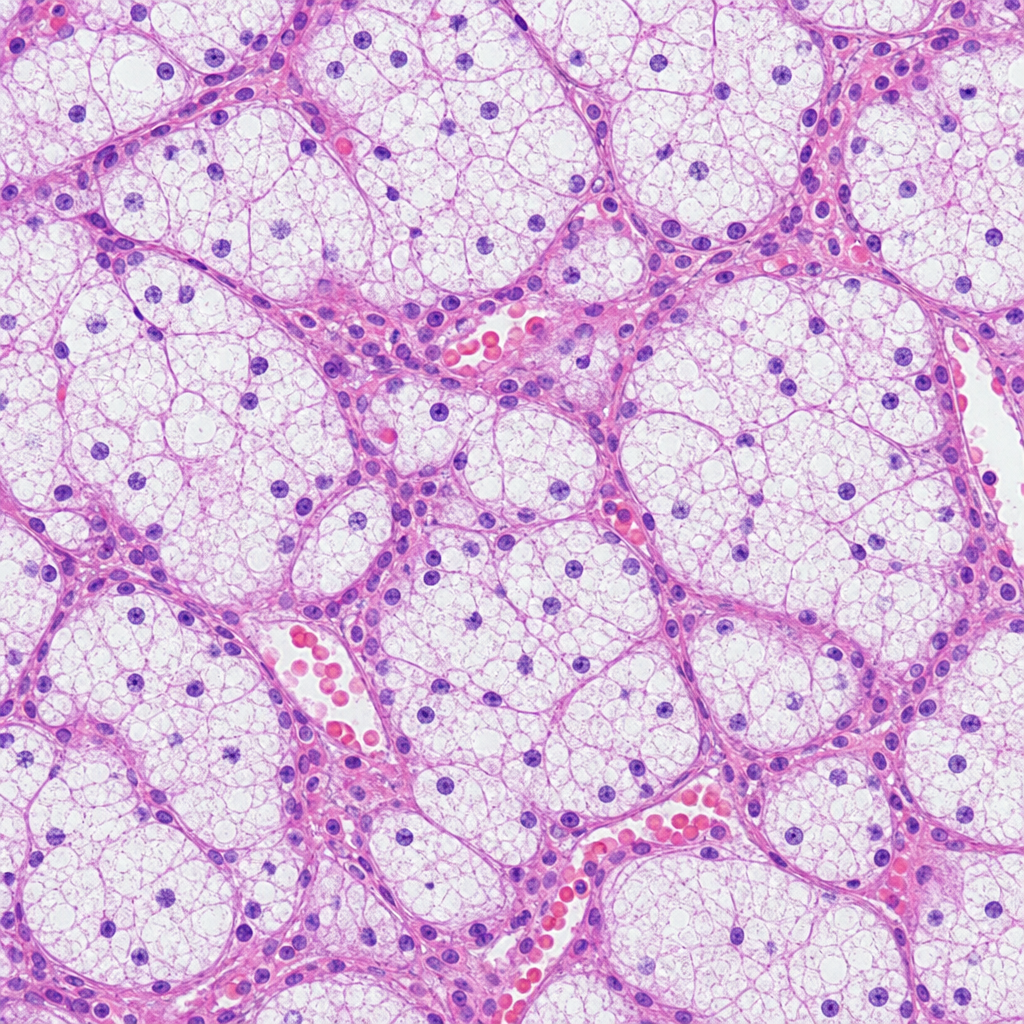
A patient presents with a renal mass leading to hematuria and flank pain. The histological image below is shown. What is the likely diagnosis?
Treatment of Renal cell carcinoma of less than 4 cm will be-
A patient presented with renal cell carcinoma invading the IVC and the renal vein. Which of the following statements is false?
Which of the following statements about hypernephroma is true?
All are true about carcinoma penis except which of the following?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app