
Urology — MCQs

On this page
Which of these is the best for management of a 3 cm stone in renal pelvis without evidence of hydronephrosis?
Bell clapper deformity (abnormal testicular fixation) predisposes to which of the following conditions?
Time cut-off for diagnosis of Priapism is?
Straining and dribbling of urine in a male infant with recurrent urinary infection should lead to the suspicion of :
In Marshall - Marchetti - Krantz (MMK) colposuspension for stress urinary incontinence, Pubocervical fascia is attached to
Le Fort's operation is done in
Which of the following is not seen in testicular carcinoma?
Reflux into grossly dilated ureter belongs to which grade of Vesicoureteric Reflux?
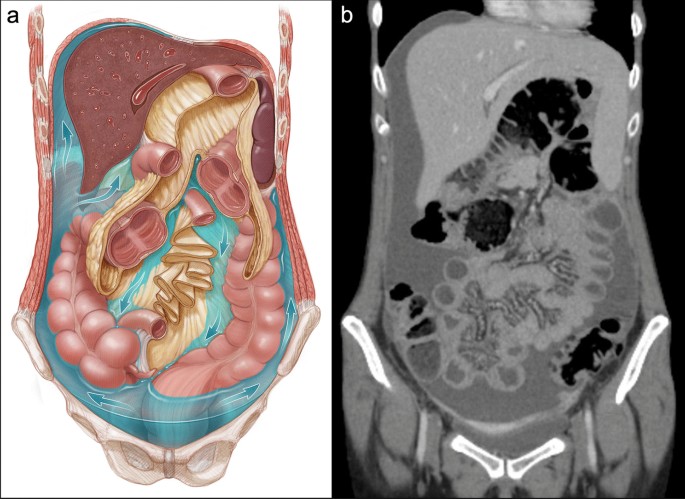
What could be the cause of the condition given in the CT below?
Which of the following is the preferred treatment for a urethral diverticulum?
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app