
Urology — MCQs

On this page
Intraoperative recognition of ureter is by which of the following features? 1. Transparent tubular appearance 2. Pale glistening appearance 3. Longitudinal vessels on surface 4. Circumferential vessels on surface Select the correct answer using the code given below:
A 22-year-old male rugby player presents with acute scrotal pain that began 2 hours ago. Physical examination shows a high-riding, tender left testis with an absent cremasteric reflex. Doppler ultrasound shows decreased blood flow to the left testis. What is the time-sensitive factor most critical to testicular salvage?
Which of the following statements is incorrect regarding vasectomy?
Tubectomy is typically performed on which part of the fallopian tube and why?
A patient presents with a penile lesion staged as T3, with clinically palpable lymph nodes. What is the most appropriate management?
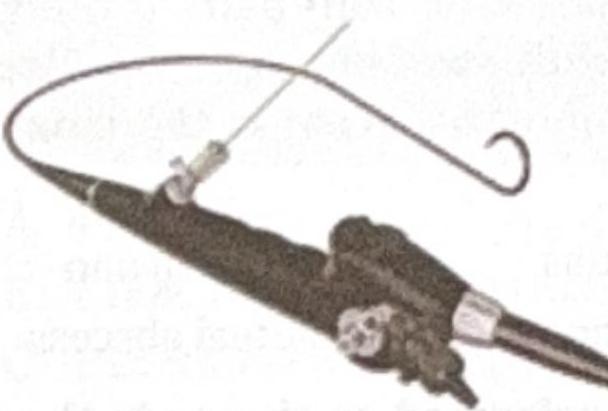
Identify the instrument shown in the image.
A 30-year-old male undergoes varicocele surgery to correct his left-sided varicocele. Following the procedure, the surgeon explains the postoperative changes to the patient. The patient asks, "Through which route does the venous drainage primarily occur after the surgery?" Which of the following is the correct response by the surgeon?
A 50 year old male patient came to the outpatient department with complaints of hematuria. A 2 x 2 cm bladder mass is seen which is low grade transitional cell carcinoma. Which among the following is the ideal management?
A 13-year-old boy is brought to the emergency department by his parents for evaluation of severe groin pain for the past 4 hours. His symptoms began while he was participating in a basketball game. On arrival to the ED, the resident on call notes a swollen, tender, and elevated left testicle with absence of the cremasteric reflex. A urology consult is requested and the patient is scheduled for surgery. An abnormality in which of the following anatomical structures is most likely responsible for this patient’s condition?
The complication which will not occur after PCNL surgery:
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app