
Urology — MCQs

On this page
A 60-year-old male smoker presents with discoloration of urine and has brought a sample to your clinic. He denies any pain or discomfort while passing urine. No history of fever is present. IVU of the patient is shown. Which is the next best investigation to be done?

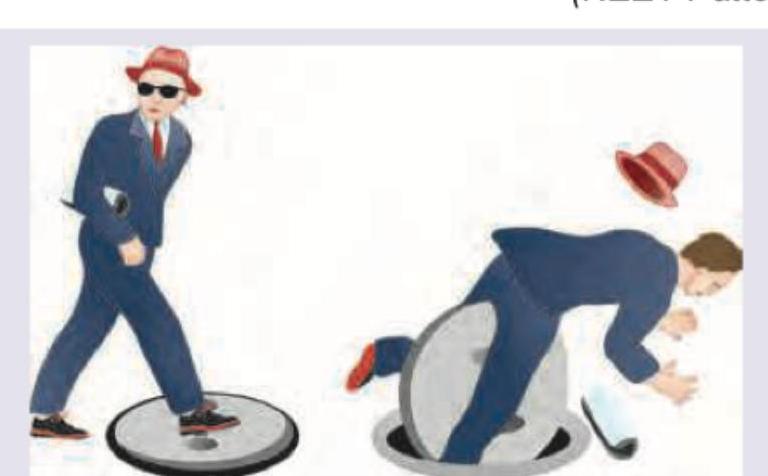
A person could not pass urine after a fall shown below. On examination vitals are stable but bladder is palpable. What is the probable diagnosis? (NEET Pattern 2018)
A 25-year-old gentleman complains of dragging pain in the scrotum. The examination reveals the scrotum full of bag of worms which disappear on lying down. The usual first line option for relief is :
Extracorporeal Shock Wave Lithotripsy (ESWL) is most commonly used for the treatment of
Anderson-Hynes plasty is a type of repair of
Which method of vasectomy has the highest failure rate ?
The most frequent complication of fracture pelvis is injury to :
Regarding varicocele, all of the following are true except :
Consider the following statements in respect of prostatic carcinoma : 1. Most originate from peripheral zone 2. Prostatic needle biopsy is better performed under trans rectal ultrasound 3. Prostate specific antigen is the specific test 4. L.H.R.H. analogues are used as medical treatment for metastatic disease Which of the statements given above is/are correct ?
A patient is diagnosed to have a Stage T3a carcinoma of the prostate. Clinically, this implies
Practice by Chapter
Urological Anatomy
Practice Questions
Hematuria Evaluation
Practice Questions
Urinary Calculi
Practice Questions
Benign Prostatic Hyperplasia
Practice Questions
Prostate Cancer
Practice Questions
Bladder Cancer
Practice Questions
Renal Cell Carcinoma
Practice Questions
Testicular Tumors
Practice Questions
Urinary Tract Infections
Practice Questions
Urinary Incontinence
Practice Questions
Genitourinary Trauma
Practice Questions
Pediatric Urology Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app